plasmacytoma







































Plasmacytomas are discrete, solitary tumors of neoplastic monoclonal plasma cells in either bone or soft tissue (extramedullary). It is a rare tumor that is associated with latent systemic disease in the majority of affected patients. In contradistinction to multiple myeloma, there is minimal or no systemic bone marrow involvement.
Solitary plasmacytomas can be divided into two groups according to location:
- solitary bone plasmacytoma (~70%)
- extramedullary plasmacytoma (~30%)
Epidemiology
- overall, solitary plasmacytoma represent 3-6% of all plasma cell neoplasia (i.e. including multiple myeloma, plasma cell leukemia)
- usually occur in patients between 40 and 80 years of age
- the median age is 55 years, that is 10 years younger than patients with multiple myeloma
Clinical presentation
The most common symptom of solitary bone plasmacytoma is pain at the site of the skeletal lesion due to bone destruction by the infiltrating plasma cell tumor.
Pathology
A plasmacytoma can arise in any part of the body. A solitary bone plasmacytoma arises from the plasma cells located in the bone marrow, whereas extramedullary plasmacytoma is thought to arise from plasma cells located in mucosal surfaces. Both represent a different group of neoplasms in terms of location, tumor progression, and overall survival rate. Both do, however, share many of the biologic features of other plasma cell disorders.
Radiographic features
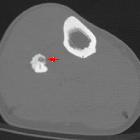
Plasmacytoma (as with multiple myeloma) are typically seen as well-defined, “punched-out” lytic lesions with associated extraosseous soft-tissue masses, similar in appearance to most metastatic lesions. In advanced plasmacytoma, there is often marked erosion, expansion, and destruction of the bone cortex, sometimes with thick ridging around the periphery, creating a “soap bubble” appearance.
CT
CT may demonstrate subtle lytic lesions or small soft-tissue masses, particularly of the sternum, that are not visible at radiography.
MRI
Use of short-inversion-time inversion recovery and contrast-enhanced fat suppression techniques may improve the sensitivity of MR imaging.
Treatment and prognosis
Treatment may consist of radiotherapy alone, surgery alone, or a combination of the two depending on location and resectability of the plasmacytoma . Solitary bony plasmacytomas are highly radiosensitive with local control rates of greater than 80% .
Three patterns of failure indicating poorer prognosis include development of multiple myeloma, local recurrence, and development of new lesions . The progression rate to multiple myeloma is higher in solitary bone plasmacytoma (65-85% at 10 years) than extramedullary plasmacytoma .
Siehe auch:
- Osteoid-Osteom
- Aneurysmatische Knochenzyste
- Osteolyse
- Riesenzelltumor
- Osteoblastom
- Knochenmetastasen
- Ostitis fibrosa cystica
- Plasmozytom des Knochens solitär
- extraossäres Plasmozytom
- Knochenmarksinfiltration bei Plasmozytom
- smoldering myeloma
- Pariser Schema Plasmozytom
- Beckenosteolysen
- International Staging System (ISS) for myeloma
- Tübinger Schema Plasmozytom
- Monoklonale Gammopathie unklarer Signifikanz
- plasmacytoma of the skeletal system
und weiter:
- Tumoren der Schädelkalotte
- Osteolysen der Kalotte
- endosteal scalloping
- Osteomyelitis
- Läsionen der Felsenbeinspitze
- verkalkte Lungenherde
- Raumforderungen des Clivus
- Pfeffer-und-Salz-Schädel
- Platyspondylie
- Superscan Szintigraphie
- Chordom
- vertebrale Metastasen
- solitäre lytische Läsion des Schädels
- moth-eaten appearance in bone
- Aseptische Wirbelkörpernekrose
- medulläre Nephrokalzinose
- Vertebra plana
- WHO-Klassifikation der Tumoren des zentralen Nervensystems
- Renale Osteodystrophie
- Knochenmetastasen des Schädels
- Amyloidose
- Autoimmunpankreatitis
- Sarkoidose ossäre Manifestationen
- cancer
- radiologisches muskuloskelettales Curriculum
- Knochentumoren
- Dens axis Zyste
- Riesenzelltumor des Knochens
- Knochenmark
- Vertebroplastie
- Läsionen des Sakrums
- musculoskeletal manifestations of sarcoidosis
- zystische Angiomatose
- Osteoklastom
- WHO classification of neoplastic diseases of lymphoid tissues
- sacrococcygeales Chordom
- pulmonale Calciphylaxie
- lytische Läsionen der Mandibula
- POEMS syndrome
- Variables Immundefektsyndrom
- lytic rib lesion (mnemonic)
- Läsionen der Mandibula
- differential diagnosis of generalized osteopaenia
- Tumoren der Wirbelsäule
- Knochenläsionen der Diaphyse
- Multiples Myelom MRT
- generalised osteopaenia
- Amyloidarthropathie
- contrast nephropathy
- polyostotic bone lesions in adults
- primary malignancies of the nasopharynx
- plasma cell dyscrasia
- Ganzkörper-Computertomographie Plasmozytom
- solitary plasmacytoma of the clivus
- testicular plasmacytoma
- primäre nasopharyngeale maligne Tumoren
- EMP
- multiple myeloma of the orbit
- nodular liver involvement in multiple myeloma
- secondary heart amyloidosis associated with multiple myeloma
- solitäres sakrales Plasmozytom
- hemorrhagic bilateral pleural effusion as first sign of IgG myeloma
- Multiples Myelom des Schädels


 Assoziationen und Differentialdiagnosen zu Multiples Myelom:
Assoziationen und Differentialdiagnosen zu Multiples Myelom: