lytische Läsionen der Mandibula



Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Stafne cyst discovered incidentally. a OPT-like reconstruction from CBCT data set showing a well-defined, unilocular radiolucency (arrow) with sclerotic borders in the region of 37 and 38. No relationship to teeth. b Axial, c coronal and d 3D reconstruction, posterior view. Bony defect (arrows) in characteristic location

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Dentigerous cyst. a OPT, b axial CT with bone windows and c dentascan reconstruction. Unilocular well-defined radiolucent lesion (thick arrows) surrounding an unerupted tooth. Immediate vicinity of the mandibular canal (dashed arrow) to the impacted tooth. d Three-dimensional reconstruction, lateral view showing the relationship of the cyst (blue), the unerupted tooth (green) and the mandibular canal (red). The cyst is attached at the level of the tooth neck and surrounds the crown. e Surgical specimen. Characteristic attachment of the cyst at the tooth neck (arrows). f Histology (haematoxylin-eosin stain, original magnification 20×): non keratinising thin epithelial lining (arrow) without rete pegs. Fibrous wall (asterisks) almost completely devoid of inflammatory cells

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Histologically proven KCOT. a OPT. Axial CT image with bone window (b) and soft tissue window (c). Multilocular well-defined radiolucent lesion (asterisk) with thin, sclerotic borders, cortical scalloping (arrow) and resorption of teeth roots. Cyst contents with attenuation values of 40–50 HU mimicking solid tissue. d Posterior view of a 3D reconstruction showing the relationship between the keratocyst (blue), the partially resorbed teeth (green) and the mandibular canal (red). The mandibular canal can be seen only in the posterior mandible, as it is encased by the keratocyst

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Basal cell nevus syndrome. a OPG. Multiple mandibular and maxillary KCOTs (asterisks) associated with impacted teeth. b Intraoperative view showing cheese-like material within the angulo-mandibular lesion (arrow). c Surgical specimen showing the KCOT (asterisk) and the associated tooth (thin long arrow). d Histology (haematoxylin-eosin stain, original magnification 40×): corrugated (dashed arrows) parakeratinised epithelium with distinct basal columnar cells with inverted polarity (arrows) and flat connective tissue interface

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Histologically proven multilocular ameloblastoma. a Axial bone window CT image. b Three-dimensional reconstruction, frontal view. c T1-weighted axial image. d T1-weighted axial image after injection of gadolinium chelates. Multilocular expansile radiolucency with characteristic “soap bubble” appearance (asterisks) and major facial deformation. Cystic components with variable signal intensity on the unenhnanced T1-weighted image suggesting variable protein content. Note variable enhancement of solid components ranging from thin enhancing walls to thick enhancing solid portions (arrows)

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Recurrent multilocular ameloblastoma. a OPT showing a well-defined, multilocular radiolucency (arrows) with sclerotic borders. b Resected specimen and c specimen radiograph clearly show bony expansion, destruction of the alveolar ridge and characteristic multilocular appearance. d Histology (haematoxylin-eosin stain, original magnification 20×): follicular ameloblastoma with squamous metaplasia (red asterisks) within follicles (arrows). Largely fibrous stroma (black asterisks) containing scattered lymphocytes

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Histologically proven eosinophilic granuloma. a OPT-like curved thick slab reconstruction, b axial CT bone window and (c) 3D reconstruction from CT data set show a well-defined radiolucent lesion (arrows) located in the angle of the mandible. Sharply delineated slightly sclerotic borders. Periosteal reaction (dashed arrow). d PET/CT showing that high FDG uptake within the posterior mandible and perimandibular soft tissues (arrow). SUVmean = 6, SUVmax = 9. e Axial T2 and f sagittal T1 after intravenous gadolinium show a large extraosseous component (arrows) with invasion of the masseter muscle. Close vicinity to the submandibulat gland. Note high signal intensity on T2 and strong enhancement after gadolinium. g Fused T2 and b 1,000 showing restricted diffusion. h ADC map showing a moderately low ADC value (ADC = 1.21 × 10−3 mm2/s, arrow) within the lesion. Note inflammatory oedema around the lesion with high ADC values (asterisk)

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Biphosphonate osteonecrosis. a OPT; b 3D reconstruction anteo-lateral view. Contrast-enhanced axial CT image with bone window settings (c) and soft tissue settings (d). Poorly defined osteolytic lesion of the left mandibular body (thick white arrows) with partly sclerotic margins (thin arrows in a) and large osseous defect (red arrows in b). Bone sequestra (dashed arrows). Associated subperiosteal phlegmon and myositis of the platysma (open arrows). e Histology (haematoxylin-eosin stain, original magnification 20×): necrotic bone (large asterisk) with inflammatory infiltration of the fatty marrow (small asterisks). Gingival mucosa (arrows)

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Osteomyelitis after tooth extraction. a OPT. b Contrast-enhanced, axial CT image with bone window settings. c Three-dimensional reconstruction. Ill-defined osteolytic area (asterisks) extending into the ascending ramus of the mandible, with cortical destruction (arrows in b and c). d Axial T1-weighted image before (d) and after (e) injection of gadolinium chelates. Hypointense signal of the mandible (arrows in d) due to marrow oedema and strong enhancement (arrows in e) due to hyperaemia. Myositis of the masseter muscle (thick dashed arrow) and streaky enhancement of the subcutaneous fat and platysma muscle (thin dashed arrow) suggesting a phlegmon. f Histology (haematoxylin-eosin stain, original magnification 20×): non-viable trabeculae (large asterisks) with bone resorption and destroyed osteoblasts. Inflammatory infiltrate (small asterisks) with neutrophils and lymphocytes as well as increased vascularisation within the fatty marrow

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. CT aspect of osteoradionecrosis 5 years after radiotherapy of a floor of the mouth SCC. a OPT. b Axial bone window CT image. c Three-dimensional reconstruction, posterior view obtained after removing the bony structures of the cervical spine. Characteristic osteolytic bone defect (arrows) with poorly defined partly sclerotic margins and soft tissue ulceration (dashed arrow). Follow-up confirmed absence of tumour

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. MRI aspect of osteoradionecrosis 2 years after chemoradiotherapy of a tonsillar SCC. a Axial T1-weighted image. b Contrast-enhanced sagittal oblique T1-weighted image and ADC map (small image in b). Bilateral hypointensity of the bony marrow. Large osseous defect with cortical destruction on the left (arrow in a). Marked, non-specific contrast enhancement, bony destruction and necrotic hypointense sequestrae (arrow in b). Note high ADC value (red circle) measured at 1.53 × 10−3 mm2/s suggesting inflammation and absent recurrence. c Macroscopic resection specimen. The necrotic area is indicated by arrows. d Histology (haematoxylin-eosin stain, original magnification 40×): necrotic bone trabeculae with inflammatory infiltrative changes in the bony marrow

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Osteoblastoma. a OPT. b Axial CT with bone window. c Sagittal oblique contrast-enhanced fat-saturated T1-weighted image. Ill-defined radiolucent lesion (arrows in a and b) with coarse sclerotic borders and calcifications (dashed arrow). Major contrast enhancement (arrow in c). d Histology (haematoxylin-eosin stain, original magnification 64×). Osteoid and woven bone (asterisk) with plump osteoblast-like cells (arrows), interposed fibroblasts and some inflammatory cells

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. SCC with mandibular invasion. Precise pre-operative assessment with MRI and PET/CT. a OPT. Poorly defined bony destruction (arrow) of the edentulous mandible. b Contrast-enhanced axial CT. Aggressive soft-tissue lesion (arrow) with secondary bone invasion. c Sagittal oblique PET/CT image. High metabolism of the tumour (black asterisk, SUVmean = 18, SUVmax = 22) and of two metastatic level I lymph nodes (arrows, SUVmean = 10, SUVmax = 15). d T2-weighted axial image. Tumour (asterisk) with marrow invasion and extensive infiltration of the floor of the mouth (dashed arrow). Note two metastatic level I lymph nodes (arrows). e The b 1,000 and f ADC map show restricted diffusion within the tumour (circle, ADC = 0.98 × 10−3 mm2/s). Variable ADC values within the metastatic lymph nodes due to the presence of necrosis (arrows in f). g Sagittal histological whole-organ slice of the resected specimen. Tumour (dashed black line) invading the mandible (black arrows) and the muscles (asterisk) of the floor of the mouth. The histological slice has the same orientation as (c)

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Condylar metastasis from adenocarcinoma. OPT (a) with osteolytic ill-defined lesion of the mandibular condyle (arrow). b Sagittal PET/CT image shows high metabolism with SUV = 12 (arrow). c Axial, contrast-enhanced, fat-saturated T1-weighted image. The infiltrative, bulky lesion invades the condyle (arrow), the internal pterygoid muscle (dashed arrow) and part of the parotid gland (thin arrow). d Intraoperative view. Extensive condylar involvement. e Histology (haematoxylin-eosin stain, original magnification 80×): large atypical polygonal cells, some with several nuclei (arrow)

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Intracystic carcinoma. a Sagittal oblique and b axial CBCT image displaying the characteristic aspect of a dentigerous cyst with well-defined cyst borders (arrows). The cyst surrounds the crown of an impacted tooth. c T2-weighted image: solid intracystic component with moderately high signal intensity (arrows). Fluid with high signal intensity within the cyst (dashed arrow). Oedema in the masseter muscle (asterisk). d ADC map with low ADC values (circle) of solid parts (ADC = 0.89 × 10−3 mm2/s) suggesting an intracystic malignant tumour despite the benign appearance on CBCT. Histology revealed SCC arising within a dentigerous cyst

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Residual cyst. a OPT. Unilocular well-defined lesion with sclerotic borders (arrow) and missing tooth 36 above. b Histology (haematoxylin-eosin stain, original magnification 20×): non-keratinised stratified squamous epithelium (arrow) with mild inflammation

Radiolucent
lesions of the mandible (differential) • Myeloma of the mandible - Ganzer Fall bei Radiopaedia

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Radicular cyst. a OPT. Unilocular radiolucent lesion with well-defined borders (asterisk) displacing teeth 33 and 34. b CT, sagittal oblique 2D MPR with bone windows. Cystic lesion surrounding the root (dashed arrow) of the non-vital tooth 34. Associated large caries with pulpal necrosis (arrow). c Histology (haematoxylin-eosin stain, original magnification 20×): fibrous connective wall containing a dense chronic inflammatory infiltrate and congested vessels (asterisk) lined by irregular non-keratinised stratified squamous epithelium. Spongiotic epithelium (arrows) penetrated by neutrophils

Mandibular
Ameloblastoma. Large bubbly lucent lesion in the mandibular body (arrows).




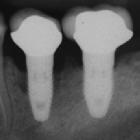
xray 2 years
after placement then 7 years later in a heavy smoker. Shows progression of periimplantitis


Mandibular
Ameloblastoma. A) Hypodense lesion in the mandibular body with cortical thining (arrows). B) A cystic extension/loculation is visible anteriorly to the right portion of the mandibular body, causing cortical bone disruption (thick arrow).

Radiolucent
lesions of the mandible (differential) • Odontogenic keratocyst - Ganzer Fall bei Radiopaedia

Mandibular
Ameloblastoma. A) and B) The cystic extension/loculation is visible anteriorly to the right mandibular body, showing an anterior enhancing septum (arrows).

Masses of
developmental and genetic origin affecting the paediatric craniofacial skeleton. Typical manifestations of nevoid basal cell carcinoma syndrome (NBCCS) in a 16-year-old boy. a Orthopantomography (OPT) shows cystic lesions of the mandible and maxilla (arrows), with unilocular and multilocular pattern and smooth or scalloped borders associated with displaced and unerupted permanent teeth. b Coronal CT scan (bone window) shows ectopic calcifications of the falx cerebri and tentorium cerebelli (arrows) and spotted meningeal calcifications (arrowheads). Brain MRI reveals a cavum veli interpositi on axial T2 (asterisk in c) and coronal contrast-enhanced T1 (asterisk in d) and also vermian dysgenesis (arrowheads in d)

Radiolucent
lesions of the mandible (differential) • Lucent lesions of the jaw (diagram) - Ganzer Fall bei Radiopaedia

Mandibular
lesions • Dentigerous cyst - Ganzer Fall bei Radiopaedia

Radiolucent
lesions of the mandible (differential) • Dental abscess extending into the submandibular space - Ganzer Fall bei Radiopaedia

Radiolucent
lesions of the mandible (differential) • Squamous cell carcinoma - mandible - Ganzer Fall bei Radiopaedia

Radiolucent
lesions of the mandible (differential) • Floating teeth - Ganzer Fall bei Radiopaedia

Radiolucent
lesions of the mandible: a pattern-based approach to diagnosis. Mandibular NHL. a OPT. Difficulty to accurately identify the lesion due its median and paramedian position and the typical anterior OPT artefact (arrowheads) masking the lesion. Subtle enlargement of the right mental foramen (long arrow) compared with the normal contralateral side (short arrow). b, c T1-weighted unenhanced axial images. d T1-weighted fat-saturated contrast-enhanced sagittal image. Large infiltrative lesion (asterisks) extending from the vestibule through the mandible into the floor of the mouth (arrows). The mandibular cortical rim is mostly preserved although the lesion shows diffuse marrow infiltration
Lucent lesions of the mandible are not uncommon and may be the result of odontogenic or non-odontogenic processes. Lucency may be conferred by a cystic process (e.g. periapical cyst) or a lytic process (e.g. mandibular metastases).
Pathology
Etiology
Odontogenic
- periapical (radicular) cyst (60% of odontogenic cystic lesions )
- periapical abscess
- dentigerous (follicular) cyst
- odontogenic keratocyst (keratocystic odontic tumor)
- ameloblastoma
- primordial cyst of the jaw
- residual cyst of the jaw
- cystic odontoma
Non-odontogenic
- fibrous dysplasia/cherubism
- mandibular metastases
- squamous cell carcinoma invading mandible
- multiple myeloma
- giant cell granuloma
- aneurysmal bone cyst
- peripheral nerve sheath tumor of mandible
- traumatic bone cyst of jaw (simple cyst)
- Stafne cyst
- brown tumor
- Langerhans cell histiocytosis
- Gorham disease
See also
Siehe auch:
- Fibröse Dysplasie
- Ameloblastom
- Multiples Myelom
- Cherubismus
- dentigerous cyst
- Keratozystischer odontogener Tumor
- Tumoren der Mandibula
- Sklerosierung Unterkiefer
- aseptische Knochenekrose der Mandibula bei Bisphosphonattherapie
- Läsionen der Mandibula
- Wurzelspitzenzysten
- Osteomyelitis der Mandibula
- Stafne-Knochenkavität
- giant cell granuloma
- aneurysmatische Knochenzyste der Mandibula
- residual cyst of the jaw
- primordial cyst of the jaw
und weiter:
- Gorlin-Goltz-Syndrom
- Osteolyse
- odontogenic myxoma
- solitary bone cyst of the mandible
- keratocystic odontic tumour
- Plattenepithelkarzinom Mandibula
- entzündliche Veränderungen Mandibula
- Osteosarkom der Mandibula
- Osteoradionekrose der Mandibula
- Periimplantitis Zahnimplantat
- intrazystisches Karzinom in der Mandibula
- Metastasen in der Mandibula


 Assoziationen und Differentialdiagnosen zu lytische Läsionen der Mandibula:
Assoziationen und Differentialdiagnosen zu lytische Läsionen der Mandibula:






aseptische
Knochenekrose der Mandibula bei Bisphosphonattherapie