Brown tumor




























Brown tumor, also known as osteitis fibrosa cystica and rarely as osteoclastoma, is one of the manifestations of hyperparathyroidism. It represents a reparative cellular process, rather than a neoplastic process. Histologically brown tumors are identical to giant cell tumor (both are osteoclastomas), and therefore, this entity can easily be misdiagnosed as such if elevated blood calcium and/or parathyroid hormone levels are not assessed for and identified.
Epidemiology
Brown tumors have a slightly greater frequency in primary than in secondary hyperparathyroidism (3% versus 2%). However, secondary hyperparathyroidism is much more common than primary hyperparathyroidism, therefore most brown tumors that are seen are associated with secondary hyperparathyroidism.
Pathology
In chronic renal disease, continual and excessive urinary calcium excretion can lower serum calcium level and lead to a rise in parathyroid hormone secretion. This results in mobilization of skeletal calcium through rapid osteoclastic turnover of bone to maintain normal serum calcium levels.
In localized regions where bone loss is particularly rapid, hemorrhage, and reparative granulation tissue, with active, vascular, proliferating fibrous tissue may replace the normal marrow contents, resulting in a brown tumor.
Hemosiderin imparts the brown color (hence the name of the lesions).
Radiographic features
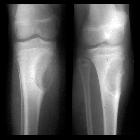
Plain radiograph
Well-defined, purely lytic lesions that provoke little reactive bone. The cortex may be thinned and expanded, but will not be penetrated.
CT
Attenuation values on CT will be in the range of blood and fibrous tissue.
Angiography (DSA)
- lesions are usually hypervascular
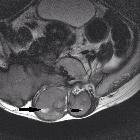
MRI
The MRI appearance depends on the relative proportion of its components. The lesions, therefore, may be solid, cystic, or mixed. Solid components are intermediate to low intensity on T1- and T2-weighted images, while the cystic components are hyperintense on T2-weighted images and may have fluid-fluid levels.
- T1 C+ (Gd): there can be enhancement of the solid component and septa
Nuclear medicine
Bone scan often shows intense uptake.
Differential diagnosis
- mnemonic for the differential diagnosis of a lucent/lytic bone lesion: FEGNOMASHIC
Siehe auch:
- Morbus Paget des Knochens
- nicht ossifizierendes Fibrom
- Aneurysmatische Knochenzyste
- Enchondrom
- Chondrosarkom
- Lucent/lytic bone lesion - differential diagnosis (mnemonic)
- intraossäres Ganglion
- Multiples Myelom
- primärer Hyperparathyreoidismus
- Chondroblastom
- Renale Osteodystrophie
- Riesenzelltumor
- Chondromyxoidfibrom
- desmoplastisches Fibrom
- Riesenzelltumor der Sehnenscheiden
- Riesenzelltumor des Knochens
- Riesenzelltumor des Sakrums
- Riesenzelltumor der Wirbelsäule
- Metastasen
und weiter:
- endosteal scalloping
- solitäre lytische Läsion des Schädels
- epiphysäre Knochentumoren
- osseous lesions preferentially involving the epiphysis
- skeletal mass with fluid-fluid levels
- central giant cell granuloma
- lytic bone lesion (mnemonic)
- Plasmozytom des Knochens solitär
- Osteoklastom
- Knochenläsionen der Epiphyse
- multiple lytic bone lesions (mnemonic)
- Knochenläsionen der Diaphyse
- Tumoren der Wirbelsäule
- Riesenzelltumor des Beckenknochens
- Engel-von-Recklinghausen-Syndrom
- Flüssigkeit-Flüssigkeitsspiegel
- multiple T2 hyperintense ossäre Läsionen
- brown tumours simulating neoplasia
- giant cell reparative cyst


 Assoziationen und Differentialdiagnosen zu Ostitis fibrosa cystica:
Assoziationen und Differentialdiagnosen zu Ostitis fibrosa cystica: