mukoepidermoides Karzinom der Speicheldrüsen









Mucoepidermoid carcinoma is a tumor that usually occurs in the salivary glands. It can mimic most other tumors of the glands, and therefore is often considered in the differential.
Epidemiology
Mucoepidermoid carcinomas are seen throughout all adult age groups but are most common in middle age (35-65 years of age) . However, it is the most common malignant salivary gland tumor of childhood . Overall, mucoepidermoid carcinomas account for :
- 2.8-15.5% of all salivary gland tumors:
- 1-10% of all major salivary gland tumors
- 6.5-41% of minor salivary gland tumors
In the parotid gland, they are the most common malignant primary neoplasm. A slight female predilection has been described, and radiation has been implicated as a risk factor .
Clinical presentation
Mucoepidermoid carcinomas most frequently arise in the parotid gland, and presents as a painless swelling, with or without facial nerve involvement. These tumors can however be found anywhere there are salivary glands. Overall distribution across various glands is as follows :
- major salivary glands: ~50% *
- parotid gland: ~40%
- submandibular gland: ~7%
- sublingual gland: ~3%
- minor salivary glands: ~50%
- palate: most common
- retromolar trigone
- floor of the mouth
- buccal mucosa
- lip
- tongue
- other: anywhere in the proximal aerodigestive tract, the lacrimal glands and even in the bronchi
As such, presentation will depend on the anatomic location.
Pathology
The tumors are composed of a mixture of:
Histology
Histology will often show clear mucin containing cells, which stain reddish pink with the mucicarmine stain. Mucoepidermoid tumors are graded histologically into:
- low grade:
- well-differentiated cells with little cellular atypia
- high proportion of mucous cells
- prominent cyst formation
- intermediate grade: intermediate features
- high grade
- poorly differentiated with cellular pleomorphism
- high proportion of squamous cells
- solid with few if any cysts
Markers
- mastermind-like 2 (MAML2) gene rearrangement
- most (around 75-80%) mucoepidermoid carcinomas are thought to harbor gene fusions involving MAML2: alteration that appears to be specific for mucoepidermoid carcinoma
Radiographic features
Radiographic appearances largely depend on grade, making preoperative imaging important in planning and counseling.
Ultrasound
Typically a well-circumscribed hypoechoic lesion, with a partial or completely cystic appearance. The lesion stands out against the relatively hyperechoic normal parotid gland.
CT
Low-grade tumors appear as well-circumscribed masses, usually with cystic components. The solid components enhance, and calcification is sometimes seen. They have appearances similar to benign mixed tumors.
High-grade tumors, on the other hand, have poorly defined margins, infiltrate locally and appear solid.
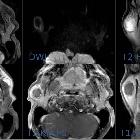
MRI
Again, imaging is dependent on grade.
Low-grade tumors have similar appearances to benign mixed tumors:
- T1: low to intermediate signal; low signal cystic spaces
- T2: intermediate to high signal; cystic areas will be high signal
- T1 C+ (Gd): heterogeneous enhancement of solid components
High-grade tumors, on the other hand, have lower signal on T2 and poorly defined margins and infrequent cystic areas:
- T1: low to intermediate signal
- T2: intermediate to low signal
It is essential to image the cranial nerves with fat-saturated post-contrast T1 sequences to assess for perineural spread, and as such the base of skull should be imaged up to and including the cavernous sinus and inner ear.
Treatment and prognosis
Treatment is dependent on grade and location:
- low grade (well-circumscribed) can usually be treated with wide local excision and preservation of the facial nerve, without the need for neck dissection or adjuvant radiotherapy
- high grade (poorly circumscribed) usually requires complete parotidectomy, often with sacrifice of the facial nerve, neck dissection (as nodal metastases are common) and adjuvant radiotherapy
Prognosis is also very dependent on grade, with low-grade tumors having a 90-98% survival and a low local recurrence rate, compared to 30-54% surviving, and a very high local recurrence rate for high-grade tumors .
Additionally, this tumor has a predilection for perineural spread, and careful and long term follow-up is therefore required.
Differential diagnosis
The differential is therefore different according to appearance.
For well-circumscribed lesions consider:
- benign mixed tumor (BMT): can be indistinguishable
- Warthin tumor
- adenoid cystic carcinoma
For infiltrative lesions consider:
- adenoid cystic carcinoma
- lymphoma (NHL)
- metastasis (especially squamous cell carcinoma metastases to intra-parotid nodes)
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu mukoepidermoides Karzinom der Speicheldrüsen:
Assoziationen und Differentialdiagnosen zu mukoepidermoides Karzinom der Speicheldrüsen: