neurogene Blase













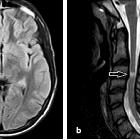
Neurogenic bladder is a term applied to a dysfunctional urinary bladder that results from an injury to the central or peripheral nerves that control and regulate urination. Injury to the brain, brainstem, spinal cord or peripheral nerves from various causes including infection, trauma, malignancy or vascular insult can result in a dysfunctional bladder .
Epidemiology
In a large cohort study, the mean age of neurogenic bladder patients was 62.5 years and resultant etiologies included :
- multiple sclerosis: ~17%
- Parkinson disease: ~15%
- cauda equina syndrome: ~9%
- paralytic syndrome: ~8%
- stroke complications: ~6%
Clinical Presentation
Depending on the location of the injury in the nervous system, patients typically present with increased frequency, nocturia, urinary incontinence/urgency, urinary tract infection and urinary retention. The bladder may be hyperreflexic, hyporeflexic or areflexic with impaired to no sensation .
Classification
A number of classification schemes exist for neurogenic bladders, including the Lapides classification which remains popular.
Radiographic features
Generally a markedly contracted or distended bladder.
Fluoroscopy/IVP
Sensory neurogenic bladder
Inability to sense bladder fullness results in a large rounded and smooth bladder. Voiding is often preserved.
Motor paralytic bladder
Atonic large bladder with the inability of detrusor contraction during voiding.
Uninhibited neurogenic bladder
Rounded bladder with a trabeculated appearance to the mucosa above the trigone from detrusor contractions. On voiding large interureteric ridge is noted
Reflex neurogenic bladder
Results from detrusor hyperreflexia with a dyssynergic sphincter. This leads to contrast extension to the posterior urethra and an elongated pointed urthera with pseudodiverticula.
Autonomous neurogenic bladder
Intermediate between detrusor hyperreflexia (contracted) and dysreflexia (atonic).
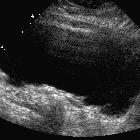
Ultrasound
Detailed images of the bladder often demonstrate a thick wall with a small contracted or large atonic bladder. A large post-void residual is often noted.
Treatment and prognosis
Depending on the etiology, various techniques can be employed to maintain renal function and prevent urinary tract infections. Self-catheterization, medication or surgical interventions including cystoplasty or sphincterotomy can be employed.
Differential diagnosis
Imaging differential considerations include:
- bladder outlet obstruction
- cystic pelvic mass
- posterior urethral valves
- myelodysplasia
See also
Siehe auch:
- Encephalomyelitis disseminata
- Morbus Parkinson
- Balkenblase
- Blasenentleerungsstörung
- Weihnachtsbaumblase
- cutaneous ileocystostomy
und weiter:


 Assoziationen und Differentialdiagnosen zu neurogene Blase:
Assoziationen und Differentialdiagnosen zu neurogene Blase: