Posterior inferior cerebellar arterial infarct













Posterior inferior cerebellar artery (PICA) occlusion may cause infarction of any part of the vascular territory of the PICA, namely the posterior inferior cerebellum, inferior cerebellar vermis, and lateral medulla.
Epidemiology
Typically considered the most common territory involved in cerebellar infarction, although at least one study has demonstrated similar frequencies of PICA and superior cerebellar artery (SCA) infarcts.
Clinical presentation
Vertigo, nausea and truncal ataxia are the most common presenting features. Signs of a lateral medullary syndrome may coexist in ~30% .
Headache and neck pain is normally the result of full posterior inferior cerebellar artery territory infarcts and is likely secondary to the associated swelling and mass effect . There are multiple eponymous posterior stroke syndromes, often presenting incompletely . Variations are common and the PICA syndrome for example, often presents with facial pain as the initial symptom and hypoalgesia, affecting either side of face .
Radiographic features
As with all cases of suspected stroke, CT or MRI is required urgently to exclude hemorrhagic stroke. CT angiography should be utilized if the patient fits thrombolysis therapy guidelines . MR angiography and CT angiography both have very high sensitivity for vessel occlusion identification, at 87% and 100% respectively . MRI is far superior to CT in the sensitivity of acute ischemic stroke across all vascular territories. In the first twenty-four hours, studies show approximately 75-95% sensitivity for MRI diffusion-weighted images, compared to CT of 16% .
Treatment and prognosis
Treatment of posterior inferior cerebellar artery, and posterior circulation strokes in general, depends upon the nature, timing, and severity of symptoms. If the timing of diagnosis fits within 4.5 hours of the onset of symptoms, then patients can be treated with thrombolysis . Acute endovascular therapies, often in the form of lysis or clot removal, can be used, particularly in basilar artery occlusion . In large volume cerebellar infarcts, neurosurgical treatment with occipital decompression or external ventricular drainage (EVD) can be lifesaving in patients who have acute hydrocephalus or raised intracranial pressure causing reduces consciousness . In PICA infarction, the outcomes are generally expected to be good .
Differential diagnosis
Due to the small confined area in the inferior aspect of the posterior cranial fossa, the swelling caused by a PICA infarct can lead to significant mass effect and midline shift which may mimic a cerebellar mass such as a primary brain tumor or metastasis.
Siehe auch:
- Ischämischer Schlaganfall
- Kleinhirninfarkt
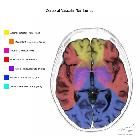
- arterielle Versorgungsgebiete des Gehirns
- Wallenberg-Syndrom
- Arteria cerebelli inferior posterior (PICA)
- Versorgungsgebiet der PICA
und weiter:


 Assoziationen und Differentialdiagnosen zu posterior inferior cerebellar artery (PICA) infarct:
Assoziationen und Differentialdiagnosen zu posterior inferior cerebellar artery (PICA) infarct:



