pulmonary arterial hypertension
























Pulmonary hypertension is defined as a resting mean pulmonary arterial pressure of 25 mmHg or greater at right heart catheterization, which is a hemodynamic feature that is shared by all types of pulmonary hypertension. A resting mean pulmonary arterial pressure of 20 mmHg or less is considered normal, while mean pulmonary arterial pressures ranging between 21-24 mmHg are considered abnormal requiring further investigation of the clinical course of the disease.
Terminology
The use of the term pulmonary arterial hypertension is restricted to those with a hemodynamic profile in which high pulmonary pressure results from elevated precapillary pulmonary resistance and normal pulmonary venous pressure and is measured as a pulmonary wedge pressure of 15 mmHg or less. This corresponds to the hemodynamic profiles of groups 3, 4, and 5 in the Dana Point classification system, which was updated during the 5th World Symposium on Pulmonary Hypertension.
Epidemiology
Epidemiology varies with the underlying cause and risk factors. Overall, there is a female predilection.
Risk factors include :
- drugs and toxins
- aminorex (withdrawn from the market)
- fenfluramine
- dexfenfluramine
- toxic rapeseed oil
- amphetamines
- L-tryptophan
- HIV infection - HIV-associated pulmonary arterial hypertension
- portal hypertension and liver disease: portopulmonary hypertension
- connective tissue disease
- scleroderma
Clinical presentation
Classical clinical presentation of pulmonary arterial hypertension is the combination of dyspnea (especially with exercise) with symptoms and signs of elevated right heart pressures, including peripheral edema and abdominal distention .
An ECG may demonstrate right ventricular strain and hypertrophy.
Pathology
Pulmonary arterial hypertension is defined as a mean pulmonary arterial pressure >25 mmHg at rest or >30 mmHg with exercise and pulmonary capillary wedge pressure ≤15 mmHg measured by cardiac catheterization . It can result from either increased pulmonary venous resistance (most common) or increased pulmonary arterial flow, such as with a left-to-right shunt .
Even in cases of increased flow, the main factor in generating severe pulmonary hypertension is an arteriopathy, which has four main components :
The earliest change is muscular hypertrophy in muscular arteries which, over time, results in changes in the more proximal arteries. Eventually, fibrosis of the wall occurs, at which point the process is irreversible .
Classification
In addition to cases of idiopathic pulmonary arterial hypertension, there are numerous known causes, and these can be subdivided in many ways. A simple unofficial classification is to divide the causes of secondary pulmonary arterial hypertension anatomically:
- chest wall and upper airways, e.g.
- kyphoscoliosis
- hypoventilation syndrome
- pulmonary veins and left heart, e.g.
- pulmonary capillaries and pulmonary parenchyma, e.g.
- pulmonary arteries, e.g.
- chronic and/or repeated pulmonary emboli
- arteritis
See: causes of pulmonary arterial hypertension for a complete list.
Alternative classifications include:
- primary and secondary pulmonary arterial hypertension (outdated)
- precapillary versus post-capillary
- 2003 3 World Symposium on Pulmonary Arterial Hypertension classification
- 2008 4 World Symposium on Pulmonary Hypertension classification : Dana Point classification of pulmonary hypertension
- 2013 5 World Symposium on Pulmonary Hypertension classification : Nice classification of pulmonary hypertension
Radiographic features
Plain radiograph
By the time the diagnosis of pulmonary arterial hypertension is made, 90% of patients have an abnormal chest radiograph although sensitivity and specificity are low . Features include:
- elevated cardiac apex due to right ventricular hypertrophy
- enlarged right atrium
- prominent pulmonary outflow tract
- enlarged pulmonary arteries
- pruning of peripheral pulmonary vessels
- radiographic correlates of underlying causes like kyphoscoliosis, valvular heart disease, or changes due to interstitial lung disease can also be noted in some cases
Echocardiography
When screening patients with a clinical suspicion of pulmonary hypertension, echocardiography findings can be used to grade the probability of elevated pulmonary artery pressures being present on right heart catheterization, as well as identify possible precipitants such as an atrial septal defect, valvular regurgitation or stenosis, or left ventricular diastolic dysfunction
The first measurement is the maximum velocity of the tricuspid regurgitant jet as observed from the apical four chambers, right ventricular inflow tract, or parasternal short (at the aortic valve level) axis views. The measured velocity informs one as follows:
- velocities >3.4 m/s are definitely abnormal, and the suspicion for pulmonary hypertension is high
- velocities below 2.8 m/s (or unmeasurable) and between 2.8 and 3.4 m/s require further measurements
- velocities <2.8 m/s (or unmeasurable) are stratified as low suspicion if there are <2 positive categories, and intermediate if there are 2 or more
- velocities between 2.8 and 3.4 m/s are either intermediate suspicion (<2 positive categories)
The ventricles (category A), pulmonary artery (category B), and right atrium and inferior vena cava (category C) may reveal suggestive findings of increased pressure/volume (a category is "positive" when one or more of the following findings are present).
The relative dimensions of the ventricles may be altered by the exaggerated interventricular dependence characteristic of elevated right heart pressures, and demonstrate
- a right ventricle:left ventricle basal diameter ratio exceeding 1.0 (RV/LV ratio >1)
- a left ventricular eccentricity index >1.1
- a manifestation of flattening of the interventricular septum, assessed by dividing the short-axis diameter of the LV parallel, and then perpendicular, to the septum and dividing these values to yield an eccentricity index
- this is often "eyeballed" as a "D sign" (a reference to the shape of the left ventricle)
The pulmonary artery diameter and pulsed/continuous wave Doppler indices are assessed in category B for the following findings
- an acceleration time (AT) of the right ventricular outflow tract <105 ms and/or mid-systolic notching of the Doppler envelope
- the latter suggestive of group 1 (precapillary) pulmonary arterial hypertension
- an early diastolic pulmonary regurgitation velocity over 2.2 m/s
- PA diameter >25 mm
Finally, the inferior vena cava and right atrium are assessed for the following features
- an inferior vena cava which is over 2.1 cm at end-expiration with <50% collapse (when an inspiratory sniff is performed)
- <20% variance with quiet breathing is also a positive finding
- right atrial area >18 cm is abnormal
- measured at end-systole
Other measures such as cardiac output and pulmonary vascular resistance are also assessed when more hemodynamic information is necessary. Ultimately, diagnosis cannot be made with echocardiography, and a right heart catheterization is needed when it would inform treatment.
CT
High-resolution CT (HRCT) chest, of course, is indispensable in assessing the lung parenchyma and to identify possible causative processes (e.g. interstitial lung disease, COPD, etc.).
In pulmonary capillary haemangiomatosis, small ill-defined centrilobular nodules and interlobular septal thickening may be apparent .
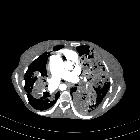
Additionally, routine CT chest and CT pulmonary angiography (CTPA) can also identify changes in the pulmonary vasculature and the heart. Features include:
Extracardiac vascular signs
- enlarged pulmonary trunk (measured at pulmonary artery bifurcation on an axial slice vertical to its long axis)
- >29 mm diameter is often used as a general predictive cut-off however, a recent study suggests :
- 31.6 mm may be a more statistically robust cut-off in patients without interstitial lung disease (specificity 93%)
- pulmonary trunk enlargement is a poor predictor of pulmonary hypertension in patients with interstitial lung disease (specificity ~40%)
- a diameter of <29 mm does not necessarily exclude pulmonary hypertension
- dilated pulmonary trunk is considered the most specific sign on CT examination
- sex-specific reference values obtained from the Framingham Heart Study suggest cut-off values 27 mm for women and 29 mm for men (on ECG-gated non-contrast CT)
- >29 mm diameter is often used as a general predictive cut-off however, a recent study suggests :
- main pulmonary artery (pulmonary trunk) to ascending aorta ratio
- higher ratio correlates with higher PA pressure
- the ratio obtained on the axial image at the bifurcation of the right pulmonary artery
- adult: normal ratio is less than 1.0
- children: normal up to a ratio of ~1.09
- enlarged pulmonary arteries
- mural calcification in central pulmonary arteries
- most frequently seen in patients with Eisenmenger phenomenon
- evidence of previous pulmonary emboli
- a segmental artery-to-bronchial diameter ratio of 1:1-1.25 or more in three or four lobes in the presence of a dilated (≥29 mm) main pulmonary artery and absence of significant structural lung disease has a specificity of 100% for the presence of pulmonary hypertension
- carina crossover sign
Cardiac signs
ECG-gated CTPA ideally required:
- right ventricular hypertrophy: defined as the wall thickness of >4 mm
- straightening or bowing (towards the left ventricle) of the interventricular septum
- right ventricular dilatation (a right ventricle–to–left ventricle diameter ratio of more than 1:1 at the midventricular level on axial images)
- decreased right ventricular ejection fraction
- ancillary features
- dilatation of the inferior vena cava and hepatic veins
- pericardial effusion
Parenchymal signs
- centrilobular ground-glass nodules
- especially common in patients with idiopathic pulmonary arterial hypertension
- pathologically: represent cholesterol granulomas, which are caused by ingestion of red blood cells by pulmonary macrophages, a result of repeated episodes of pulmonary hemorrhage
- neovascularity: tiny serpiginous intrapulmonary vessels that often emerge from centrilobular arterioles but do not conform to usual pulmonary arterial anatomy: can be seen as a manifestation of severe pulmonary hypertension
Mediastinal signs
MRI
MRI and MR angiography have an increasing role in the management of pulmonary arterial hypertension, as dynamic imaging of both the heart and pulmonary circulation can be achieved.
Angiography
Traditionally pulmonary angiography has been the gold standard to identify small peripheral occlusions and to better quantify the degree of stenosis. Increasingly this has been replaced by better quality CTPA and cardiac CT.
Care needs also to be taken when performing a pulmonary angiogram in patients with severe pulmonary hypertension.
Treatment and prognosis
Medical therapy includes :
- calcium channel antagonists
- nitric oxide
- prostanoids, e.g. epoprostenol, treprostinil, iloprost
- endothelin antagonists e.g. bosentan, sitaxentran, ambrisentan
- phosphodiesterase inhibitors e.g. dipyridamole
In selected cases, combined heart and lung transplantation can be performed . In patients with very high right heart pressures, an atrial septostomy has also been performed but is associated with high immediate mortality and reduces oxygenation due to the right-left shunt formed.
In cases where pulmonary arterial hypertension is due to proximal pulmonary emboli, a pulmonary thromboendarterectomy is a surgical option.
Despite extensive research and recent advances in medical management prognosis remains poor, with a mean survival of only three years in untreated patients . Patients typically succumb to right heart failure or sudden death.
Differential diagnosis
- pulmonary arterial dilatation can occur in the absence of pulmonary hypertension in some people with pulmonary fibrosis
- for an enlarged pulmonary artery also consider - idiopathic dilatation of the pulmonary trunk
As a broad differential on plain film consider:


 Assoziationen und Differentialdiagnosen zu pulmonale Hypertonie:
Assoziationen und Differentialdiagnosen zu pulmonale Hypertonie:

