Rückenmarksinfarkt

Location,
length, and enhancement: systematic approach to differentiating intramedullary spinal cord lesions. Spinal cord infarction. An 82-year-old female with hypertension and hyperlipidaemia presents with acute bilateral lower extremity weakness. a Axial T2 image demonstrates a large cross-sectional area of hyperintensity (arrow) within the thoracic cord. b Axial CT angiogram image shows mural thrombus within the aorta (arrow) at the same level of the spinal cord findings with no appreciable filling of the lumbar arteries. Sagittal T2 (c), DWI (d) and ADC (e) images reveal a long-segment intramedullary lesion in the lower cord (arrows) that is T2 hyperintense and has restricted diffusion

a schematic
diagram showing anatomical signification of uncomplete cord injuries

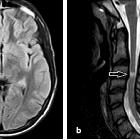
Spinal cord
infarction presenting as Brown-Séquard syndrome from spontaneous vertebral artery dissection: a case report and literature review. a Sagittal T2-weighted magnetic resonance image of cervical spine reveals spinal cord enlargement with hyperintense lesion at the level of C1–3 (red arrow). b Axial T2WI shows hyperintense signal of right spinal cord (red arrow). This is consistent with spinal cord infarction (SCI). (c)(d) HR-MRI VISTA sequence shows narrowing of the right vertebral artery at the level of C1–3 with eccentric high signal parallel to the narrowed lumen (red arrow)

Spinal cord
infarction presenting as Brown-Séquard syndrome from spontaneous vertebral artery dissection: a case report and literature review. Post-treatment image (a) After 3 months of therapy, Sagittal T2-weighted magnetic resonance image of cervical spine shows the range of abnormal signal of spinal cord in level C1–3 diminished. (b)(c) HR-MRI VISTA reexamination shows that lumen recanalization of the right vertebral artery

Spinal cord
infarction presenting as Brown-Séquard syndrome from spontaneous vertebral artery dissection: a case report and literature review. Spinal cord arerial supply. The arteries supplying the spinal cord include the anterior spinal artery (ASA), the posterior spinal artery (PSA), and the radicular artery. The upper region (C1-T2 segments) of the spinal cord is supplied mainly by the vertebral artery. Starting at the level of C3, the anterior and posterior spinal arteries receive a branch from the vertebral artery, that of the radicular artery. In our case, the basic lesion of this patient is the occlusion of the cervical radicular artery caused by vertebral artery dissection, which eventually resulted in right spinal cord infarction

Acute spinal
cord ischemia syndrome • Spinal cord ischemia - Ganzer Fall bei Radiopaedia

Acute spinal
cord ischemia syndrome • Acute spinal cord ischemia - Ganzer Fall bei Radiopaedia

Artery of
Adamkiewicz • Spinal cord ischemia - Ganzer Fall bei Radiopaedia

Acute spinal
cord ischemia syndrome • Spinal cord infarct - Ganzer Fall bei Radiopaedia

Ventral cord
syndrome • Spinal cord infarct - Ganzer Fall bei Radiopaedia
Rückenmarksinfarkt
Siehe auch:
- Transverse Myelitis
- Encephalomyelitis disseminata
- Ventriculus terminalis
- spinales Hämangioblastom
- central cord syndrome
- Brown-Séquard-Syndrom
- intramedulläre spinale Tumoren
- Arteria-spinalis-anterior-Syndrom
- Adamkiewicz-Arterie
- Akute disseminierte Enzephalomyelitis
- anterior cord syndrome
- Blutversorgung Rückenmark
- HIV myelitis
- CMV myelitis
- hämorrhagischer spinaler Infarkt
- Sarkoidose Rückenmark
- systemic lupus erythematosus of myelon
und weiter:


 Assoziationen und Differentialdiagnosen zu Rückenmarksinfarkt:
Assoziationen und Differentialdiagnosen zu Rückenmarksinfarkt: