subfalzine Herniation



Subfalcine herniation, also known as midline shift or cingulate hernia, is the most common cerebral herniation pattern. It is generally caused by unilateral frontal, parietal or temporal lobe disease that creates a mass effect with medial direction of the ipsilateral cingulate gyrus beneath the free edge of the falx cerebri due to raised intracranial pressure.
Radiographic features
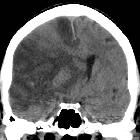
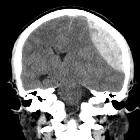
CT
The easiest method of evaluating for subfalcine shift is a straight line drawn in the axial plane, at the level of the foramen of Monro, and measuring the distance between this line and the displaced septum pellucidum. The shift of the septum pellucidum from this midline can be measured in millimeters and compared over time to determine any change.
In more severe hernias, the displaced tissue may compress the corpus callosum and contralateral cingulate gyrus as well as the ipsilateral lateral ventricle, foramen of Monro, causing dilation of the contralateral lateral ventricle.
Subfalcine hernias occur anteriorly, as the anterior falx (although rigid) is displaced, secondary to mass effect. The posterior falx, on the other hand, is more rigid and will resist the displacement.
MRI
Findings are best visualized on coronal MR imaging. Unilateral mass effect from pathology in the frontal, parietal or temporal region, such as intracranial hemorrhage or tumor, causes displacement of the brain away from the mass.
Treatment and prognosis
Complications
- hydrocephalus due to obstruction of the foramen of Monro
- anterior cerebral artery (ACA) territory infarct due to compression of ACA branches, specifically the pericallosal artery
- focal necrosis of the cingulate gyrus due to direct compression against the falx cerebri
ACA infarction occurs as the cingulate sulcus extends under the falx dragging the ipsilateral anterior cerebral artery with it. If this becomes compressed against the falx, distal anterior cerebral artery infarction can occur, the most common clinical manifestation being contralateral leg weakness.
In subfalcine herniation, the degree of midline shift correlates with the prognosis; less than 5 mm deviation has a good prognosis, whereas a shift of more than 15 mm is related to a poor outcome .
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu subfalzine Herniation:
Assoziationen und Differentialdiagnosen zu subfalzine Herniation: