Thymic epithelial tumors


































Thymic epithelial tumors are rare tumors arising from thymus in anterior mediastinum of middle age patients. However, they are still the most common primary neoplasm of the thymus and anterosuperior mediastinum. This article discusses thymomas, invasive thymomas and thymic carcinoma.
Epidemiology
The typical presentation is in the 5 to 6 decades, without gender predilection .
Clinical presentation
Thymic epithelial tumors are, in the vast majority of cases, located in the anterior mediastinum, although cases in the neck and posterior mediastinum have been reported . As such, they can present with venous obstruction, dysphagia or stridor.
Associations
Over 30 conditions have been associated with thymomas . Those with the strongest correlation and most frequently encountered include:
- myasthenia gravis: most common association
- 10-20% of patients with myasthenia gravis have a thymoma
- 30-50% of patients with a thymoma have myasthenia gravis
- pure red cell aplasia
- 50% of patients with pure red cell aplasia have a thymoma
- 5% of patients with a thymoma have pure red cell aplasia
- hypogammaglobulinaemia
- 5% of patients with hypogammaglobulinaemia have a thymoma
- 10% of patients with a thymoma have hypogammaglobulinaemia
- systemic lupus erythematosus (SLE)
- rheumatoid arthritis
- non-thymic cancers
Pathology
Macroscopically thymic tumors are of variable shape, with thymomas typically rounded with a bosselated outer surface. The cut surface is tan or grey-pink with lobulated architecture, separated by fibrous septae .
Both non-invasive and invasive thymomas may appear to have an intact capsule, and microscopic examination is required. Obvious macroscopic invasion may be evident .
Larger tumors are more likely to demonstrate cystic changes as well as hemorrhage and calcification.
Numerous histologic classification systems for thymic epithelial neoplasms have been proposed over the years. A widely used, and simple division is into :
- non-invasive thymoma
- invasive
The WHO classification scheme for thymic epithelial tumors divides them according to histological appearance, which correlates with the likelihood of invasiveness (from least to most likely) and thus correlate with staging . The Masaoka staging system is commonly adopted to assess invasion and is assessed at surgery .
Location
The vast majority of thymomas arise in their expected anterior mediastinal region. Very rarely they can arise at other sites in around 4% of cases (e.g. cervical deeper mediastinal region) - see ectopic thymoma .
Radiographic features
Plain radiograph
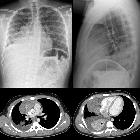
Presents as an anterior mediastinal mass. On plain radiographs, they are often seen as a well-defined, lobulated soft tissue density slightly towards one side of the mediastinum. Can demonstrate associated calcification (commonly amorphous/flocculent).
CT
Thymic epithelial tumors are usually of soft tissue attenuation and are usually located between the sternum and great vessels. A cystic component is common and calcification can be seen in as high as 10-50% of patients which tends to be small and more commonly peripherally located. Although calcifications are most commonly seen in more malignant types of thymic neoplasm, individually they are not considered a discriminatory finding. Of interest, CT findings can predict histology as described by the WHO classification scheme for thymic epithelial tumors and thus by extension prognosis .
- type A: tumors (medullary histology thymomas), are typically rounded, smooth or somewhat lobulated masses of soft tissue attenuation
- type B: tumors more frequently demonstrate calcification, although calcification is also frequently seen in thymic carcinoma
- type C:
- tumors (thymic carcinoma) usually demonstrate an invasion of mediastinal fat or mediastinal structures and are usually much larger than type A or B tumors
- mediastinal lymph node enlargement may be present although the reported frequency of this finding varies widely (13-44%)
Pleural seeding is seen in invasive thymoma or thymic carcinoma.
MRI
- T1: isointense to slightly hyperintense signal compared to muscle
- T2
- heterogeneous signal, slightly higher than muscle
- cystic areas may be seen, especially in larger tumors
- fibrous septa crossing the mass are of low signal intensity
- in/out phase imaging: typically no signal drop out, i.e. no chemical shift
- T1 C+ (Gd): linear regions of enhancement may be seen coursing through the mass, thought to represent fibrous septae
Nuclear medicine
Thymic carcinoma has higher FDG-18 PET-CT uptake than other, better differentiated thymic epithelial tumors, as well as normal or hyperplastic thymus. Using an SUV cutoff point of 5.0 high sensitivity (84.6%) and specificity (92.3%) can be achieved when trying to distinguish between thymic carcinoma and thymoma .
Treatment and prognosis
Treatment depends on the stage as well as the presence of myasthenia gravis, which dictates earlier surgical excision . For thymoma, local excision usually suffices, and complete excision usually results in cure. For invasive thymoma, surgery may still be contemplated if complete excision is thought possible. If not, then down-staging with preoperative chemotherapy may be employed .
Surgical resection can be achieved via a number of approaches :
- sternotomy
- video-assisted thoracoscopic thymectomy
- transcervical thymectomy (limited exposure)
Radiotherapy is not usually employed for stage I thymomas but has a role in both postsurgical management of resected invasive thymoma or for inoperable invasive tumors, including thymic carcinoma .
Prognosis is significantly influenced by the histological type and surgical staging (e.g. Masaoka staging system).
- type A, AB and B1 tumors have the best survival (up to 85% 5-year survival)
- type B2 and B3 tumors have intermediate survival
- type C tumors (thymic carcinoma) have the worst survival (35% 5-year survival)
Recurrence rates after surgical excision vary between 8-29% depending on the series and type of tumor .
Differential diagnosis
The differential for plain radiography is that of an anterior mediastinal mass.
On cross-sectional imaging (CT/MRI), the differential is usually narrowed down to:
- primary tumors of the thymus
- thymic rebound, e.g. postchemotherapy
- thymic hyperplasia
- lymphoma: primary thymic lymphoma or involvement from systemic lymphoma
- mediastinal germ cell tumors
See also
Siehe auch:
- Tumoren des vorderen oberen Mediastinums
- Thymuskarzinom
- systemischer Lupus Erythematodes
- Thymushyperplasie
- Myasthenia gravis
- invasives Thymom
- mediastinale Keimzelltumoren
- Tumoren des Thymus
- Myasthenia gravis Thymom
- WHO Klassifikation der Thymome
- Staging Thymome nach Masaoka
- Masaoka staging system
- WHO classification scheme for thymic epithelial tumours
- nicht invasives Thymom
- pure red cell aplasia
- Hypogammaglobulinämie
und weiter:


 Assoziationen und Differentialdiagnosen zu Thymom:
Assoziationen und Differentialdiagnosen zu Thymom:




