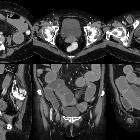
Dünndarmileus bei inkarzerierter Schenkelhernie






Dünndarmileus bei inkarzerierter Schenkelhernie
Schenkelhernie Radiopaedia • CC-by-nc-sa 3.0 • de
Femoral hernias (alternative plural: herniae) are a type of groin herniation and comprise a protrusion of a peritoneal sac through the femoral ring into the femoral canal, posterior and inferior to the inguinal ligament. The sac may contain preperitoneal fat, omentum, small bowel, or other structures.
Epidemiology
There may be an increased right-sided predilection . There is an increased prevalence in females .
Pathology
Most femoral hernias protrude inferior to the course of the inferior epigastric vessels and medial to the common femoral vein. They often have a narrow funnel-shaped neck and may compress the femoral vein, causing engorgement of distal collateral veins.
Occasionally, a femoral hernia may develop differently or be located somewhere besides medially to the femoral vessels. Possibilities include a hernia developing through the lacunar ligament (Laugier's hernia), or through the pectineal fascia (Cloquet's hernia) . Femoral hernias in an atypical relation to the femoral vessels include those lateral (Hesselbach's hernia), prevascular (Velpeau's hernia) or retrovascular (Serafini's hernia) .
Radiographic features
Ultrasound
Scanning below the inguinal ligament, assessing the space medial to the femoral vein for a hernia. The Valsalva maneuver can be performed to provoke herniation; the common femoral vein should also dilate .
CT
Femoral hernias typically have a characteristic funnel-shaped neck.
On axial CT images, the neck of the femoral hernia sac may be seen as a narrow protrusion through the femoral ring just medial to the common femoral vein. This can often look indented and compressed by the hernia sac.
Coronal images can also be very useful and it is usually seen in the space containing the fat pad between the inguinal ligament, common femoral vein and adductor longus muscle . Assessment of compression of the femoral vein and any distal engorgement should be made.
Differential diagnosis
The main differential is made with inguinal hernias. Femoral hernias are more common in women and unlike inguinal hernias, they remain lateral to the pubic tubercle. Femoral hernias invariably compress the femoral vein, while it is rare for an inguinal hernia to compress the femoral vein.
See also
- abdominal hernias
- pantaloon hernia
- De Garengeot hernia: femoral hernia containing an appendix
Dünndarmileus Radiopaedia • CC-by-nc-sa 3.0 • de
Small bowel obstruction (SBO) accounts for 80% of all mechanical intestinal obstruction, the remaining 20% results from a large bowel obstruction. It has a mortality rate of ~5%.
Clinical presentation
Classical presentation is cramping abdominal pain and abdominal distension with nausea and vomiting. Radiographic findings can be evident 6-12 hours before the onset of clinical symptoms .
Pathology
Etiology
Causes can be divided into congenital and acquired. Acquired causes may be extrinsic causing compression, intrinsic, or luminal.
In developed countries, adhesions are by far the most common cause, accounting for ~75% of obstructions while in developing countries incarcerated hernias are much more common accounting for 80% of obstructions .
Congenital
- jejunal atresia
- ileal atresia or stenosis
- enteric duplication
- midgut volvulus
- mesenteric cyst
- Meckel diverticulum
Extrinsic causes
- fibrous adhesions
- main cause in developed countries (75% of cases)
- almost all are related to post-operative adhesions with a small percentage secondary to peritonitis
- diagnosis of exclusion as adhesive bands are not seen on CT
- abrupt change in caliber without mass lesion, inflammation or bowel wall thickening at transition point
- abdominal hernia
- 10% of cases in developed countries
- external hernia related to abdominal or pelvic wall defect (congenital weakness or previous surgery)
- internal hernia with protrusion of viscera through peritoneum or mesentery into another abdominal compartment
- endometriosis
- rare cause of SBO
- endometrial implants are typically on anti-mesenteric edge of the bowel
- solid enhancing nodule contiguous with or penetrating the thickened bowel wall
- may infiltrate the submucosa with a hypoattenuating layer between the muscularis and mucosa
- masses
- extrinsic neoplasm
- intra-abdominal abscess
- aneurysm
- hematoma
Intrinsic bowel wall causes
- inflammation, e.g. Crohn, tuberculosis, eosinophilic gastroenteritis
- small bowel obstruction in Crohn disease may relate to:
- acute flare with luminal narrowing secondary to transmural inflammation
- cicatricial stenosis in long-standing disease
- adhesions or incisional hernias from previous surgery
- small bowel obstruction in Crohn disease may relate to:
- tumor (rare)
- primary small bowel neoplasms are rare (<2% all GI malignancy) and usually advanced at the time of SBO.
- GIST, adenocarcinoma, lymphoma
- asymmetric and irregular mural thickening at the transition point
- small bowel involvement of metastatic disease is more common
- peritoneal carcinomatosis with an extrinsic serosal disease in association with the transition point
- cecal malignancy involving ileocecal valve
- primary small bowel neoplasms are rare (<2% all GI malignancy) and usually advanced at the time of SBO.
- radiation enteritis
- produces adhesive and fibrotic changes in the mesentery with luminal narrowing and dysmotility
- may cause an obstruction in the late phase (>1 year after therapy)
- intestinal ischemia
- occlusion or stenosis of the mesenteric arterial or vascular supply
- produces small bowel wall thickening and obstruction
- pneumatosis and portal venous gas if advanced
- intramural hematoma
- trauma, iatrogenic, anticoagulant therapy, Henoch-Schonlein purpura
- produces luminal narrowing
- better seen on non-enhanced CT with homogenous, regular and spontaneously hyper-attenuating wall
- intussusception
- rare in adults (<5% of SBO)
- lead point may relate to neoplasm, adhesion or foreign body
- bowel-within-bowel with or without mesenteric fat and mesenteric vessels
- leading mass should be carefully interpreted and differentiated from the soft-tissue pseudotumor that represents the intussusception itself
Intraluminal causes
- swallowed, e.g. foreign body, bezoar
- gallstone ileus
- rare complication of recurrent cholecystitis
- biliary-intestinal fistula with impaction of a gallstone in the small bowel
- meconium ileus (or meconium ileus equivalent, distal intestinal obstruction syndrome)
- migration of gastric balloon
Radiographic features
Abdominal radiograph
Abdominal radiographs are only 50-60% sensitive for small bowel obstruction . In most cases, the abdominal radiograph will have the following features:
- dilated loops of small bowel proximal to the obstruction (see 3-6-9 rule)
- predominantly central dilated loops
- three instances of dilatation > 2.5 - 3 cm
- valvulae conniventes are visible
- gas-fluid levels if the study is erect, especially suspicious if
- >2.5 cm in width
- in the same loop of bowel but at different heights (> 2 cm difference in height)
However, obstruction (which may be high-grade mechanical obstruction) may also present with the following features:
- gasless abdomen: gas within the small bowel is a function of vomiting, NG tube placement and level of obstruction
- string-of-beads sign: small pockets of gas within a fluid-filled small bowel
Ultrasound
Bedside test help to diagnose small bowel obstruction, findings suggestive of small bowel obstruction :
- dilated bowel loop (diameter > 3 cm)
- ineffective peristalsis
- results in "to-and-fro" or "whirling" appearance of intra-luminal contents
- prominence of the valvulae conniventes
- present in dilated jejunal loops
Extent of obstruction is typically implied rather than sought directly based on the involvement of the ascending/descending colon, the morphology of the small bowel loops (high mucosal folds pattern present in the jejunum, absent in the ileum), and involvement of the stomach. Findings suggestive of bowel ischemia/infarction (will need urgent surgical evaluation):
- extraluminal free fluid
- the "pointy" triangular appearance of inter-loop free fluid is often referred to as the tanga sign
- loss of peristalsis
- bowel wall thickening >3 mm
- with effacement of mural architecture
- mural gas
CT
CT is more sensitive than radiographs and will demonstrate the cause in ~80% of cases . Features on CT may include:
- dilated small bowel loops >2.5 cm up from outer wall to outer wall
- normal caliber or collapsed loops distally
- small bowel feces sign
Closed-loop obstructions are diagnosed when a bowel loop of variable length is occluded at two adjacent points along its course. May be partial or complete with characteristic features:
- radial distribution of several dilated, fluid-filled bowel loops
- stretching of prominent mesenteric vessels converging towards the point of torsion
- U-shaped or C-shaped configuration
- beak sign at site of fusiform tapering
- whirl sign reflecting rotation of bowel loops around a fixed point
Strangulation is defined as closed-loop obstruction associated with intestinal ischemia. Mainly seen when the diagnosis is delayed (up to 10% of small bowel obstructions) and associated with high mortality. Features are non-specific and include:
- thickened and increased attenuation of the bowel wall
- halo or target sign
- pneumatosis intestinalis
- portal venous gas
- localized fluid or hemorrhage in the mesentery
Positive oral contrast is not usually necessary for the diagnosis of small bowel obstruction :
- usually, becomes dilute in the setting of SBO and does not usually reach the transition point before the scan occurs
- may obscure the evaluation of the small bowel wall, limiting evaluation of bowel ischemia
Some literature sources recommend Gastrografin (diatrizoate meglumine) to shorten the postoperative course of those with non-operative small bowel obstruction .
See also
Siehe auch:
- Schenkelhernie
- Dünndarmileus
- inkarzerierte Schenkelhernie
- Dünndarmileus bei inkarzerierter Leistenhernie
- Dünndarmileus durch Obturatorhernie
und weiter:


 Assoziationen und Differentialdiagnosen zu Dünndarmileus bei inkarzerierter Schenkelhernie:
Assoziationen und Differentialdiagnosen zu Dünndarmileus bei inkarzerierter Schenkelhernie:

