PUJ obstruction











































Pelviureteric junction (PUJ) obstruction/stenosis, also known as ureteropelvic junction (UPJ) obstruction/stenosis, can be one of the causes of obstructive uropathy. It can be congenital or acquired with a congenital pelviureteric junction obstruction being one of the commonest causes of antenatal hydronephrosis.
Epidemiology
It may present in both pediatric and adult populations although they tend to have differing etiology. The estimated incidence in pediatric populations is ~1 per 1,000-2,000 newborns, and there is a male predominance (M:F = 2:1).
Clinical presentation
Many cases are asymptomatic and identified incidentally when the renal tract is imaged for other reasons. When symptomatic, symptoms include recurrent urinary tract infections, stone formation and even a palpable flank mass. They are also at high risk of renal injury even by minor trauma.
Classically intermittent pain after drinking large volumes of fluid with a diuretic effect is described, due to the reduced outflow from the renal pelvis into the ureter .
Pathology
Pelviureteric junction obstruction is most commonly unilateral but is reported to be bilateral in ~30% (range 10-49%) of cases . There is a recognized predilection towards the left side (~67% of cases).
During embryogenesis, the pelviureteric junction forms usually around the fifth week and the initial tubular lumen of the ureteric bud become recanalized by ~10-12 weeks. The pelviureteric junction area is the last to recanalize. Inadequate canalization is thought to be the main embryological explanation of a pelviureteric junction obstruction. Extrinsic obstructions secondary to bands, kinks, and aberrant vessels also are commonly encountered.
Interestingly, research has failed to identify any anatomically-discrete pelviureteric junction although physiologically there is evidence of a sphincter-like action in this region .
Etiology
- congenital (neonatal)
- idiopathic and often unknown; proposed causes include
- abnormal muscle arrangement at the pelviureteric junction
- anomalous collagen collar at pelviureteric junction
- ischemic insult to pelviureteric junction region
- urothelial ureteral fold
- extrinsic ureter compression or encasement
- crossing vessel (at pelviureteric junction)
- idiopathic and often unknown; proposed causes include
- adult
- preceding renal pelvic trauma
- obstructing calculus immediately distal to pelviureteric junction
- previous pyelitis with scarring
- intrinsic malignancy, e.g. upper tract urothelial carcinoma
- extrinsic ureter compression or encasement
- fibrosis
- crossing vessel (at pelviureteric junction)
- malignancy
- aortic aneurysm
Associations
- in congenital cases, some renal tract abnormalities are recognized
- in ~40% of cases, an aberrant, accessory, or early-branching lower pole segment vessel is found and observed to compress the ureter, causing mechanical obstruction
Radiographic features
Fluoroscopy/IVU
Traditionally intravenous urography/pyelography (IVP/IVU) has been performed for assessing for pelviureteric junction obstruction. The administration of furosemide may be used to assist in confirming the diagnosis, in particular, to exclude a dilated non-obstructed upper collecting system (so-called 'baggy pelvis').
Ultrasound
- will often show a dilated renal pelvis with a collapsed proximal ureter
- Doppler sonography: the obstructed kidneys may show higher resistive indices
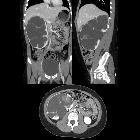
CT
May show evidence of hydronephrosis +/- caliectasis with collapsed ureters. Useful for assessing crossing vessels at the pelviureteric junction, especially when surgical intervention is planned .
Renal scintigraphy
Renal scintigraphy can quantitate the degree of obstruction:
Treatment and prognosis
Treatment depends on the underlying cause. In a majority of congenital cases, the condition is benign, and usually, no intervention is required. However, when there is a definitive structural obstruction (commonly adult cases), surgical intervention with pyeloplasty or stenting may be necessary.
Differential diagnosis
General imaging differential considerations include:
- congenital megacaliectasis
- central renal pelvis tends to be relatively collapsed
- extrarenal pelvis
- calyces are not prominently distended
- parapelvic cyst
- when multiple can be indistinguishable on US or non-contrasted CT
- IVP confirms normal pelvicalyceal system in between the cysts
Siehe auch:
- Hydronephrose
- Obstruktive Uropathie
- Hydronephrose Gradeinteilung
- Ureterabgangsstenose Klassifikation
- ureteral stricture
- Megakalikose
- congenital ureteropelvic junction obstruction
und weiter:


 Assoziationen und Differentialdiagnosen zu Ureterabgangsstenose:
Assoziationen und Differentialdiagnosen zu Ureterabgangsstenose:

