Battered-Child-Syndrom





























Suspected physical abuse (SPA), also known as non-accidental injury (NAI) or inflicted injury, in infants and young children represents both ethical and legal challenges to treating physicians.
Radiologists may be the first clinical staff to suspect non-accidental injuries when confronted with a particular injury pattern. Knowledge of these is essential if the opportunity to save a child from future neglect is not to be missed. At the same time, it is essential that suspicion is not raised inappropriately as the consequences for an innocent but accused parent or guardian are significant.
Terminology
Over recent years, there have been a number of titles given to the constellation of injuries that are the result of the physical abuse of children. Whilst "Non-Accidental Injury (NAI)" is ubiquitous, Suspected Physical Abuse (SPA) and Inflicted Injury (II) are the preferred terms .
Epidemiology
In 2001 an estimated 903,000 children were victims of maltreatment including:
- neglect: 57%
- physical abuse: 19%
- cutaneous injury: most common
- fractures are noted in ~30% (range 11-55%)
- sexual abuse: 10%
- psychological maltreatment: 7%
- medical neglect: 2%
Clinical presentation
A number of features have been recognized as suspicious:
- injury in the non-ambulatory/totally dependent child
- injury and history given are inconsistent
- delay in seeking medical attention
- multiple fractures with no family history of osteogenesis imperfecta
- retinal hemorrhage
- torn frenulum
- history of household falls resulting in fracture
- despite falls being common, fractures are uncommon
Specific injuries
- abdominal injuries
- thoracic injuries
Radiographic features
Skeletal injuries
A skeletal survey is performed in cases of suspected abuse to assess and document the extent of skeletal injuries. The so-called babygram (whereby the entire baby is imaged in one view) is not an acceptable substitute due to the overall lower quality that it produces; each anatomical region requires different radiographic exposures to accurately image.
Lead markers should be used in skeletal surveys and some institutions will repeat radiographs that do not have a lead marker within the primary field.
Bone scans are performed in some institutions because of their ability to detect radiographically-occult fractures.
Specific fractures
A number of fractures have been recognized as highly specific to non-accidental injuries (rather than accidental injury). They include:
- metaphyseal fracture (so-called bucket handle fracture or corner fracture)
- present in up to 39-50% of abused infants <18 months
- said to be virtually pathognomonic of NAI
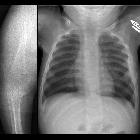
- rib fractures
- especially posterior ribs
- may have no overlying bruising
- although vigorous cardiopulmonary resuscitation can occasionally cause anterior rib fractures, posterior rib fractures do not occur
- costochondral junction injuries and/or fractures
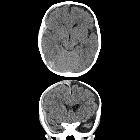
- skull fracture: suspicious features include:
- non-parietal skull fracture (a parietal fracture is more suggestive of accidental injury)
- involves multiple bones
- diastatic sutures
- crosses sutures
- depressed fracture (fracture a la signature)
- scapular fractures
- sternal fractures
- outer third clavicular fractures
Fractures which are moderately specific for NAI are :
- bilateral fractures with fractures of differing ages
- digital fractures in non-ambulant children
- vertebral fractures or vertebral subluxation
- spiral humeral fractures
- separation of epiphysis
- complex skull fractures
Fractures which have low specificity for NAI are :
- middle clavicular fractures
- linear simple fractures of parietal bone
- single fractures in diaphysis (spiral humeral fracture is an exception)
- greenstick fractures
Skeletal scintigraphy
It is the most sensitive in detecting fractures of rib, scapula, spine, diaphysis and pelvis. The test becomes positive few hours after injury. Normally there is high uptake in the epiphyses of bones which should not be confused with a fracture .
Dating injuries
The ability to date injuries is critical for medicolegal purposes and thus must be done carefully (please refer to specialist text for specific guidelines).
Traumatic periosteal injury can be seen up to 7 days post-injury (and therefore can be used for dating). Traumatic periosteal injuries can be seen on diaphyseal and rib injuries. Diaphyseal injuries start healing after one week. Healing should be complete by 12 weeks. Rib fractures are often missed, hence current practice is to repeat chest films in two weeks to observe any healing fractures. .
Metaphyseal (and costochondral junction) injuries do not heal with periosteal reaction and if visible are less than four weeks old. Skull fractures also do not heal with periosteal reaction and if seen are less than two weeks old.
Practical points
- skeletal dysplasias: one of the major - albeit uncommon - pitfalls in diagnosing NAI (e.g. Schmid-type metaphyseal chondrodysplasia, osteogenesis imperfecta I and IV), which may lack the florid features of the full-blown disease and can be easily confused with NAI
- features to differentiate osteogenesis imperfecta from NAI include
- the presence of osteopenia
- bowing or remodeling of bones
- the presence of Wormian bones
- features to differentiate osteogenesis imperfecta from NAI include
- growth plates can also cause a degree of confusion, most notably at the hip, base of the fifth metatarsal, elbow and the acromion
- birth injuries
- rickets
Siehe auch:
- Osteogenesis imperfecta
- subdurales Hämatom
- Sternumfraktur
- Scapulafraktur
- Schädelfraktur
- Wormsche Knochen
- metaphyseal fracture
- kindliche Rippenfrakturen
- Leipziger Schema
- non parietal skull fracture
- non-accidental skeletal injuries
und weiter:
- kindliche Schädelfraktur
- Infantile kortikale Hyperostose
- Duodenalhämatom
- CHILD-Syndrom
- Osteogenesis imperfecta Typ 3
- Glutarylazidurie Typ 1
- MRT des Neugeborenen - Gehirn
- bucket handle fracture
- Osteogenesis imperfecta Typ 1
- Deprivationssyndrom
- non-accidental trauma - abdominal manifestations
- anterior rib fractures
- Toddler-Fraktur Kleinkind-Fraktur
- physiologische Periostreaktion des Neugeborenen
- diastatische Schädelfraktur


 Assoziationen und Differentialdiagnosen zu Battered-Child-Syndrom:
Assoziationen und Differentialdiagnosen zu Battered-Child-Syndrom:





