Osteogenesis imperfecta





































Osteogenesis imperfecta (OI) refers to a heterogeneous group of congenital, non-sex-linked, genetic disorders of collagen type I production, involving connective tissues and bones.
The hallmark feature of osteogenesis imperfecta is osteoporosis and fragile bones that fracture easily, as well as, blue sclera, dental fragility and hearing loss. There is extreme variation in clinical symptoms based on genetic basis and subtypes. Osteogenesis imperfecta affects both bone quality and quantity (i.e. bone mass).
Epidemiology
The estimated incidence is approximately 1 in every 12,000-15,000 births . Osteogenesis imperfecta occurs with equal frequency among males and females and across races and ethnic groups. The lifespan varies with the type (see osteogenesis imperfecta classification).
Clinical presentation
The clinical presentation of osteogenesis imperfecta is highly variable, ranging from a mild form with no deformity, normal stature and few fractures to a form that is lethal during the perinatal period.
In general, four major clinical features characterize osteogenesis imperfecta :
Other features include ligamentous laxity and hypermobility of joints, short stature and easy bruising.
Pathology
A fundamental pathology in osteogenesis imperfecta is a disturbance in the synthesis of type I collagen, which is the predominant protein of the extracellular matrix of most tissues. In bone, this defect results in osteoporosis, thus increasing the tendency to fracture. Besides bone, type I collagen is also a major constituent of dentin, sclerae, ligaments, blood vessels and skin .
Genetics
Osteogenesis Imperfecta is the result of a mutation in one of the two genes that carry instructions for making type 1 collagen. Mutations in the COL1A1 and COL1A2 genes, which encode the α2 and α2 polypeptide chains , are responsible for more >90% of all cases.
Depending on the type, the inheritance of the disorder can be autosomal dominant (>95%), autosomal recessive (<10%) or by sporadic mutation
Classification
The first classification of osteogenesis imperfecta was by Looser, in 1906 who divided the condition into two forms, osteogenesis imperfecta congenita (also known as Vrolik disease) and osteogenesis imperfecta tarda (also known as Ekman-Lobstein disease).
Since then newer classification systems were based on work by Sillence and colleagues in 1979, have taken into account the phenotypic features and the mode of inheritance. This has since been revised and up to eight forms of osteogenesis imperfecta have been identified.
Three main types are easily distinguished
Types IV to VIII are variable in severity and uncommon (see osteogenesis imperfecta classification for further detail).
Associations
Radiographic features
Plain radiograph
This is the preferred initial examination.
- head, neck and spine
- basilar invagination
- wormian bones
- kyphoscoliosis
- vertebral compression fractures
- codfish vertebrae
- platyspondyly
- chest
- pectus excavatum or carinatum
- accordion ribs
- pelvis
- general
- severe osteoporosis
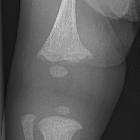
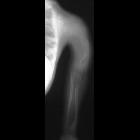
- deformed, gracile (over-tubulated) bones
- cortical thinning
- hyperplastic callus formation
- popcorn calcification: the metaphyses and epiphyses exhibit numerous scalloped radiolucent areas with sclerotic margins
- zebra stripe sign: cyclic bisphosphonate treatment produces sclerotic growth recovery lines in the long bones
- formation of pseudarthrosis at sites of healing fractures
Prenatal ultrasound
The prenatal sonographic features are often useful in type II (perinatal) and type III forms.
- may show decreased calvarial ossification
- this may result in visualization of fetal brain detail
- the skull may deform/compress with transducer pressure
- may show evidence of fractures
- long bones may appear shortened and/or angulated as a result
- there may be a sonographic gap along the length of a long bone
- ribs may have a beaded appearance
- there may be the presence of polyhydramnios
CT
While showing most of the plain film features, CT may also better demonstrate:
MRI
- can be used to assess the extent of basilar invagination
Treatment and prognosis
Prognosis is very variable depending on type ranging from being uniformly lethal from type II to a slight reduction in life expectancy for type I.
Management options for non-lethal types include:
- surgical correction of deformities and the prevention of fractures
- intramedullary rods with osteotomy are used to correct severe bowing of the long bones
- intramedullary rods are also recommended for children who repeatedly fracture long bones
- different types of rods (surgical nails) are available to address issues related to surgery, bone size, and the prospect for growth; the two major categories of rods are telescopic and non-telescopic
- bisphosphonates
- growth hormone therapy
Differential diagnosis
General considerations on pediatric plain films include:
- suspected physical abuse (previously termed non-accidental injury, NAI)
- osteopenia of prematurity
- osteomalacia
- juvenile osteoporosis
- hypophosphatasia
- rickets
- Menkes syndrome (or kinky-hair syndrome)
Siehe auch:
- Biegungsbruch
- Battered-Child-Syndrom
- Osteogenesis imperfecta Typ 2
- Menkes-Syndrom
- Hypophosphatasie
- Verbiegung der langen Röhrenknochen
- Osteogenesis imperfecta Typ 3
- Osteogenesis imperfecta Typ 1
- Klassifikation Osteogenesis imperfecta
- Osteogenesis imperfecta Typ Levin
- Osteogenesis imperfecta Typ 5
- Osteogenesis imperfecta Typ 4
- Osteogenesis imperfecta Typ 6
- Osteogenesis imperfecta Typ 7
und weiter:
- Rippenusuren
- Platyspondylie
- Basiläre Impression
- Ektasie Aorta ascendens
- Rachitis
- Aseptische Wirbelkörpernekrose
- Protrusio acetabuli
- Vertebra plana
- Wormsche Knochen
- popkornartige Verkalkungen
- Ausdünnung der Kalotte
- Skelettdysplasie
- Duraektasie
- Thanatophore Dysplasie
- Tibiaverbiegung bei Kindern
- Akranie
- Gefäßverkalkungen
- Platybasie
- paediatric curriculum
- basilar invagination (mnemonic)
- lethal skeletal dysplasias
- Erweiterung des interpedunculären Abstands
- hereditary connective tissue disease
- differential diagnosis of osteoporosis
- zebra stripe sign
- Grisel-Syndrom
- perinatal lethal hypophosphatasia
- gracile bones (mnemonic)
- Erweiterung der Symphysis pubica
- zapfenförmige Epiphyse
- Idiopathische juvenile Osteoporose
- osteogenesis imperfecta and bisphosphonate lines
- fetale Rippenfrakturen
- prenatal sonographic diagnosis of osteogenesis imperfecta


 Assoziationen und Differentialdiagnosen zu Osteogenesis imperfecta:
Assoziationen und Differentialdiagnosen zu Osteogenesis imperfecta:


