Behçet disease (CNS manifestations)






CNS manifestations of Behçet disease, also known as neuro-Behçet disease, corresponds to the neurological involvement of the systemic vasculitis Behçet disease and has a variety of manifestations.
For a discussion of the disease, in general, please refer to Behçet disease article.
Epidemiology
CNS involvement is seen in 4-49% of patients with systemic Behçet disease and has the same predilection of patients of middle eastern and Japanese descent .
Clinical presentation
In the vast majority of cases, ulcerative lesions preceded neurological involvement, aiding in the diagnosis. In 3% of cases, central nervous system manifestations occur first, making diagnosis significantly more challenging . Signs and symptoms include :
- headaches
- sensory disturbances
- personality changes
- dysarthria
- cerebellar signs
Pathology
Neuro-Behçet disease, depending on the stage or degree of the inflammation, shows perivascular infiltration of leukocytes and microglia, degeneration of oligodendroglia, and perivascular softening or necrosis .
Radiographic features
Neuro-Behçet disease has a wide variety of manifestations in the central nervous system, including :
- focal or multifocal lesions
- meningoencephalitis
- cerebral vein thrombosis
Meningoencephalitis and cerebral vein thrombosis are discussed separately in general articles related to these conditions.
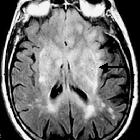
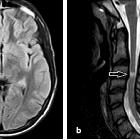
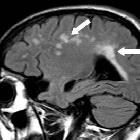
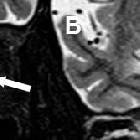
MRI
Lesions in neuro-Behçet disease typically involve , in order of preference:
- brainstem: most common, and typically in the pons
- basal ganglia: bilateral in one-third of cases
- thalamus
- subcortical white matter: less common
- spinal cord: less common
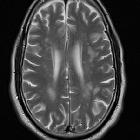
Lesions in neuro-Behçet disease typically demonstrate the following signal characteristics :
- T1: usually hypointense
- T2:
- usually hyperintense
- associated with vasogenic edema
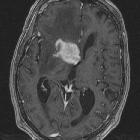
- in acute phase, lesions cause mass effect
- T1 C+ (Gd): typically moderate patchy enhancement
- DWI: isointense to slightly hyperintense
- MRS: drop in NAA, with elevated lipid and choline/creatine ratio
Treatment and prognosis
- corticosteroids: intravenous methylprednisolone infusion then oral prednisone
- immunosuppression: azathioprine, methotrexate, and TNFα inhibitors
Differential diagnosis
General imaging differential considerations include
- multiple sclerosis
- neurosarcoidosis
- primary CNS lymphoma
- gliomatosis cerebri
- antiphospholipid syndrome
- Sweet syndrome
Consider other causes of T2 hyperintensity of the basal ganglia.
Siehe auch:
- Gliomatosis cerebri
- Neurosarkoidose
- T2 hyperintense Basalganglien
- Encephalomyelitis disseminata
- primäres ZNS-Lymphom
- Morbus Behçet
- Antiphospholipid-Syndrom
und weiter:


 Assoziationen und Differentialdiagnosen zu Morbus Behçet ZNS-Manifestationen:
Assoziationen und Differentialdiagnosen zu Morbus Behçet ZNS-Manifestationen: