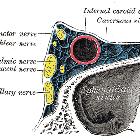
carotid-cavernous fistula













Caroticocavernous fistulas (CCF) represent abnormal communication between the carotid circulation and the cavernous sinus. They can be classified as direct or indirect which are separate conditions with different etiologies.
Epidemiology
Direct CCFs are often secondary to trauma, and as such the demographics reflect the distribution of head trauma, most commonly seen in the young male patients. The presentation is acute and symptoms develop rapidly.
In contrast, indirect CCFs have a predilection for the postmenopausal female patient and the onset of symptoms is often insidious.
Other conditions that predispose to increased risk include:
Clinical presentation
- pulsatile exophthalmos: ~75%
- chemosis and subconjunctival hemorrhage
- proptosis
- progressive visual loss: 25-32%
- pulsatile tinnitus (usually objective)
- raised intracranial pressure
- subarachnoid hemorrhage, intracerebral hemorrhage, otorrhagia, epistaxis: ~5%
- cranial nerve (III, IV, Vc, VI) palsies
Pathology
Classification
Caroticocavernous fistulas can be classified in according to various features:
Of these, vascular anatomy is most frequently used and most broadly divides caroticocavernous fistulas into two main types:
- direct: direct communication between intracavernous ICA and cavernous sinus
- indirect: communication exists via branches of the carotid circulation (ICA or ECA)
The Barrow classification of caroticocavernous fistulas further characterizes fistulas according to angiographic features:
- type A: direct connection between the intracavernous internal carotid artery and cavernous sinus
- type B: dural shunt between intracavernous branches of the internal carotid and cavernous sinus
- type C: dural shunts between meningeal branches of the external carotid artery and cavernous sinus
- type D: type B + type C
Pathophysiology
Direct (Barrow type A)
A direct fistula is due to direct communication between the intracavernous internal carotid artery and the surrounding cavernous sinus. There are a number of causes, however, aneurysm rupture and trauma are by far the most common:
- ruptured intracavernous carotid artery aneurysm
- trauma (including surgery/angiography)
- other causes include
- collagen deficiency syndromes
- fibromuscular dysplasia
- arterial dissection
Indirect (Barrow types B, C, D)
Indirect fistulas are due to communication by multiple branches between the internal and/or external carotid arteries and the cavernous sinus. The most frequent are type C, with meningeal branches of the external carotid forming the fistula .
They are postulated to occur secondary to cavernous sinus thrombosis with revascularization and thus are similar to dural arteriovenous fistulas elsewhere. Other predisposing factors appear to be pregnancy, surgical procedures in the region, and sinusitis .
Radiographic features
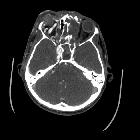
CT
CT angiography is the noninvasive imaging modality of choice for evaluation of suspected caroticocavernous fistula . Features include
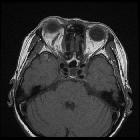
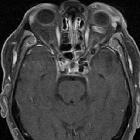
- orbital congestion
- proptosis/exophthalmos
- retrobulbar fat stranding/edema
- enlargement of extraocular muscles
- venous engorgement and enhancement
- enlarged superior ophthalmic vein
- bulging cavernous sinus
- asymmetric enhancement of cavernous sinus with attenuation similar to that of internal carotid artery and higher than that of transverse sinus
- dehiscent internal carotid artery (for direct type fistulas): snowman appearance of fistula tract involving the feeding carotid artery and draining venous pouch
- intracranial hemorrhage from a ruptured cortical vein
Angiography (DSA)
Catheter-based digital subtraction angiography is the gold standard imaging technique due to its superior spatial and temporal resolution.
- rapid shunting from internal carotid artery to cavernous sinus
- enlarged draining veins
- retrograde flow from cavernous sinus, most commonly into the ophthalmic veins
Ultrasound
- arterialized ophthalmic veins may be seen on Doppler study
Treatment and prognosis
The natural history of caroticocavernous fistulas is highly varied, ranging from spontaneous closure to rapidly progressive symptoms. As such therapy is similarly variable ranging from conservative expectant management to emergent endovascular or surgical intervention.
Conservative management
As a proportion of low flow caroticocavernous fistulas spontaneously close initial conservative management of ocular symptoms is often first employed provided no high-risk features (e.g. aneurysms of feeding vessels) or severe ocular or intracranial complications are present .
Carotid compression therapy
In addition to conservative measures, carotid-jugular compression (at the level of the carotid bulb) can be useful in the treatment of indirect fistulas resulting in closure in up to 30% of cases, presumably due to progressive thrombosis due to intermittent stagnation of blood adjacent to existing clot. In contrast, it is only successful in 17% of direct fistulas, presumably due to the higher flow through larger defect . It is important that atherosclerotic disease of the carotid bifurcation needs is excluded prior to the commencement of compression . Patients are instructed to compress the carotid bulb for 10 seconds four to six times an hour . Compression should be performed with the contralateral hand so that if symptomatic hemispheric ischemia occurs the transient paralysis results in cessation of compression.
Endovascular
Endovascular management is the mainstay of treatment for patients that fail or are not suitable for conservative management and compression therapy .
Two main approaches are available, depending on the anatomy of the fistula: transarterial embolization or transvenous embolization.
Direct fistulas
Treatment of direct fistulas requires the occlusion of the tear in the internal carotid artery. This can be achieved in a variety of ways :
- transarterial covered stent of flow-diverting stent placement in the internal carotid artery
- transarterial placement of a detachable balloon through the defect into the cavernous sinus
- transarterial or transvenous coil or other embolic material placed through the defect obliterating the cavernous sinus
- transarterial occlusion of the internal carotid artery
Indirect fistulas
Indirect fistulas require either transarterial occlusion of feeding arterial branches and/or transvenous occlusion of the cavernous sinus . Transvenous access can be challenging and may require access via the superior ophthalmic vein (sometimes with the aid of surgical exposure), inferior ophthalmic vein, lateral pterygoid plexus, superior petrosal sinus . Occasionally flow-diverting stents can be used to treat indirect fistulas if no other transarterial or transvenous approaches are available .
Surgical
Surgical treatment is relegated in most institution for cases where endovascular management is unsuccessful or impossible. Treatment may involve ligation or trapping of involved arterial segments
Complications
Spontaneous hemorrhage can be subarachnoid hemorrhage, intracerebral hemorrhage or extracranial hemorrhage (e.g. epistaxis or otorrhagia).
Ocular complications are also common and often one of the driving factors in embarking upon treatment.
Siehe auch:
- Arteria carotis externa
- Arteria carotis interna
- Intrazerebrale Blutung
- Subarachnoidalblutung
- Fibromuskuläre Dysplasie
- Ehlers-Danlos syndrome
- Sinus cavernosus
- Exophthalmus
- pulssynchrones Ohrgeräusch
- pulsatiler Exophthalmus
- caroticocavernous fistula classification
- endovascular treatment of a caroticocavernous fistula
und weiter:


 Assoziationen und Differentialdiagnosen zu Carotis-Sinus-cavernosus-Fistel:
Assoziationen und Differentialdiagnosen zu Carotis-Sinus-cavernosus-Fistel: