femoroacetabular impingement (FAI)






























Femoroacetabular impingement (FAI) refers to a clinical syndrome with clinical signs and symptoms of painful, limited hip motion resulting from certain types of underlying morphological abnormalities in the femoral head-neck region and/or acetabulum. FAI can lead to early degenerative disease.
Epidemiology
Femoroacetabular impingement is common in active young and middle-aged adult individuals, with pincer morphology being more common in middle-aged women and cam morphology more common in young men .
Risk factors
- high impact sport activity, especially in adolescence during physeal closure
- overuse activity
- previous slipped capital femoral epiphysis or Perthes disease
- coxa profunda, protrusio acetabuli
- acetabular retroversion
- posttraumatic deformities
Associations
- osteoarthritis of the hip
- cam morphology
- pincer morphology
- mixed cam/pincer morphology
- os acetabuli
Clinical presentation
Patients usually present with motion or position related to hip and/or groin pain e.g. a painfully restricted range of motion during hip flexion, internal rotation and adduction. Sometimes the pain is also described in the buttock, back or thigh and in addition, there may be symptoms of stiffness, clicking, locking, catching .
A common clinical test for femoroacetabular impingement is the FADIR test, which is sensitive but not specific .
Complications
- labral tear
- chondrolabral separation
- chondral injury e.g. carpet lesion
- osteoarthritis of the hip
Pathology
Femoroacetabular impingement is an intra-articular or internal form of impingement, where structural changes combined with dynamic factors as repetitive abnormal contact of the acetabulum and the femoral head-neck junction lead to mechanical stress and shear forces on the labrum and chondral surfaces and subsequent damage .
Etiology
The etiology of cam and pincer morphology comprises primary (idiopathic) and secondary (developmental, traumatic and iatrogenic) causes .
Subtypes
Two basic structural factors or subtypes of the femoroacetabular morphology have been identified, which can lead to femoroacetabular impingement either alone or in combination:
- cam-type: the loss of sphericity leads to shear forces at the chondrolabral junction during hip flexion and internal which can then lead to chondrolabral separation and chondral delamination typically in the anterosuperior aspect of the acetabulum
- pincer type: focal or global acetabular over-coverage can lead to labral compression and chondral wear at the site of impingement also frequently anterosuperiorly with concomitant chondral injury posteroinferiorly as a contrecoup lesion as a longterm sequel
- mixed type: a combination of the two morphologies
Location
The morphological change in cam morphology is situated at the femoral head-neck junction, most often in the anterosuperior position lateral to the physeal scar with decreased femoral head-neck offset .
Acetabular over-coverage in pincer morphology can be global or focal and concerns the acetabular rim, focal acetabular overcoverage can be anywhere but most often is also located anterosuperior due to acetabular retroversion, posterior wall prominence and os acetabuli being other forms of focal overcoverage .
Labral injuries and tears are most frequently located at the most prominent site of cam and/or pincer morphology, which is most frequently at the anterosuperior portion of the acetabular rim. Chondral contrecoup lesions in case of pincer morphology are often found posteroinferiorly .
Radiographic features
For initial evaluation of the acetabulum plain radiographs of the pelvis are recommended and an additional view of the femoral neck such as Dunn views, cross-table lateral, frog-leg lateral or Meyer lateral for the assessment of the femoral head-neck junction .
Cross-sectional imaging is advised for better characterization, the detection of chondral and labral lesions and preoperative planning .
Plain radiograph
The plain anterior-posterior radiograph of the pelvis can be evaluated for the following radiographic signs of cam and /or pincer morphology. It is important that it is acquired with neutral tilt, centered on the pubic symphysis since some of those signs will be falsely positive or negative depending with increasing tilt and rotation :
- lateral center-edge angle, acetabular index: to confirm acetabular overcoverage
- ilioischial line: coxa profunda, protrusio acetabuli
- crossover sign, ischial spine sign: acetabular retroversion
- posterior wall sign: prominent posterior wall or acetabular retroversion
- pistol grip deformity: cam morphology
In addition, several lateral hip projections including Dunn 45° and 90° views, Meyer lateral, frog-leg lateral, Lequesne's false profile, cross-table lateral have been described to assess the hip in a second plane, with the following signs :
- anterior center-edge angle (on false profile view): to confirm acetabular overcoverage
- femoral head-neck offset: cam morphology
CT
Osseous morphological abnormalities of the acetabulum and femoral head-neck junction that is possible pincer and/or cam morphology can be easily and fast assessed in multiple planes including radial (double oblique) reconstructions along the femoral neck . In addition, 3D reconstructions enable surgical planning e.g. for osteochondroplasty .
Typical findings on CT are an osseous bump in the anterosuperior position of the femoral head-neck junction with cysts and herniation pit as indirect signs for cam morphology. Increased acetabular depth, acetabular ossicle and acetabular retroversion indicate pincer morphology .
Findings can be objectified with the following measurements:
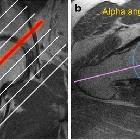
- alpha angle: >55° in anterior and >60° in anterosuperior position indicate cam morphology
- femoral head-neck offset: <6-7mm in anterosuperior position indicates cam morphology
- acetabular retroversion: (normal 12-20°) as an indicator for pincer morphology
MRI
Similar to CT MRI allows the assessment of cam and/or pincer morphology. A 3D sequence of the hip in question can be considered, for easy and fast radial (double oblique) reformations along the femoral neck and proper evaluation of the acetabulum.
In addition to morphological assessments of the femoral head-neck junction and the acetabulum and measurements as acetabular retroversion, alpha angle and femoral head-neck offset MRI allows for assessment of concomitant labral and chondral injuries like chondrolabral separation or carpet lesion and/or features indicative of the latter e.g. paralabral cysts .
MR/CT arthrography
Direct MR arthrography can improve the detection of chondral injuries as carpet lesions and can add sensitivity for the detection of labral injury e.g. tears or chondrolabral separation . Both 3D gradient-echo and spin-echo sequences have been described with good diagnostic accuracy . It seems as if CT-arthrography is most accurate in detecting labral tears .
Radiological reporting
A report for preoperative evaluation should include the following :
- description of abnormalities in the femoral head-neck junction: e.g. bump, cysts, herniation pit
- description of acetabular morphology: e.g. coxa profunda, acetabular retroversion
- associated findings e.g. bone marrow edema
- labral detachment and other labral pathology
- chondral lesions e.g. carpet lesion, chondral wear and/or defects
- measurements: e.g. alpha angle, femoral head-neck offset, acetabular index, acetabular depth
- femoral anteversion
- signs of early osteoarthritis: subchondral sclerosis, cysts, osteophytes
- associated soft tissue injuries: musculotendinous injury
Treatment and prognosis
Untreated femoroacetabular impingement can lead to damage to the labrum and acetabular cartilage, manifesting as hip and groin pain if left untreated and will later progress to early osteoarthritis of the hip.
Therapeutic management includes conservative treatment, rehabilitation and/or surgery depending on the extent of clinical signs and symptoms as well as the underlying morphology and overall patient condition. Conservative measures include activity and/or lifestyle modifications, nonsteroidal anti-inflammatory drugs, watchful waiting, whereas rehabilitation is targeted on alleviating symptoms by improving neuromuscular control and movement patterns as well as stability of the hip . Surgical options aim at restoring hip morphology and repair or reconstruction of chondral and labral damage with arthroscopic and open surgical approaches, the latter including femoral or acetabular osteotomy or osteochondroplasty . The indication for surgery warrants not only morphological changes but also typical clinical signs and symptoms indicative of femoroacetabular impingement .
Differential diagnosis
- osteoarthritis of the hip
- osteonecrosis of the hip
- other forms of hip impingement
- transient osteoporosis of the hip
- subchondral insufficiency fractures
See also
Siehe auch:
- Arthrose
- Labrumläsion Hüfte
- femoroacetabulares Impingement vom Cam-Typ
- femoroazetabuläres Impingement (Pincertyp)
- Alphawinkel Nötzli
- Femoro-acetabuläres Impingement gemischter Typ
- zentraler Osteophyt des Acetabulums
und weiter:


 Assoziationen und Differentialdiagnosen zu Femoro-acetabuläres Impingement:
Assoziationen und Differentialdiagnosen zu Femoro-acetabuläres Impingement:
