fibrocartilaginous embolism
Fibrocartilaginous embolism (also known as nucleus pulposus embolism) is a rare cause of spinal cord ischemia due to embolization of nucleus pulposus material from intervertebral disc in a retrograde direction into a spinal artery or vein.
Fibrocartilaginous embolism is a diagnosis of suspicion. Certain clinical findings make the diagnosis more likely, such as antecedent minor trauma, an absence of vascular risk factors, spinal cord imaging consistent with evolving infarction, normal CSF fluid analysis and exclusion of other possible etiologies .
Epidemiology
Fibrocartilaginous embolism seems to be more common in females (M:F 1:2.2) . Increased incidence appears to be bimodal, observed around adolescence (may be due to a common blood supply to the spinal cord and nucleus pulposus in early life) and older age (may be related to neo-vascularization that takes place in a degenerated disc) . Minor trauma appears to be the precipitating factor .
Interestingly, although rare in humans, fibrocartilaginous embolism is far more frequently encountered in veterinary practice, and is quite common in dogs .
Clinical presentation
The clinical presentation depends upon the level of the spinal cord involved. Presentation includes sudden pain in the back of the neck, often after Valsalva maneuver or physical exertion, followed by progression of signs and symptoms indicating spinal infarction . The interval from onset of pain to maximal neurological deficit ranges from 15 minutes to 48 hours .
Pathology
Increased pressure within an intervertebral disc, such as results from results from axial loading (e.g. lifting) combined with simultaneous Valsalva maneuver is thought to be responsible for the embolus . Disc material has been identified in spinal arteries and arterioles, and veins and venules . Three mechanisms of embolism have been described in the literature so far:
- intervertebral disc material herniates into the vertebral body (also known as Schmorl nodes) and then embolized to the spinal cord by retrograde venous flow, noting that the spinal venous plexus is valveless
- traumatic rupture of the annulus fibrosus, followed by tearing of the adjacent radicular artery with extrusion of nucleus pulposus material into the artery
- "injection" of disc material into arteries of the disc space, with further retrograde migration into a radicular artery
Radiographic features
Radiographic features are those of spinal cord ischemia.
Most commonly (70%) the cervical cord is affected, followed by the conus medullaris (20%), and if arterial is usually in the anterior spinal artery territory (anterior two-thirds of the cord) .
Angiography of spinal arteries can be performed to demonstrate a thromboembolic event if a vascular event is highly suspected.
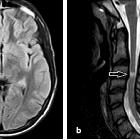
An MRI finding of cord swelling associated with a collapsed disc space at the appropriate level, in a corresponding clinical setting, should strongly suggest, if not prove, the diagnosis of fibrocartilaginous embolism .
When the embolism is venous, infarction tends to be a complete transverse spinal cord infarct .
Treatment and prognosis
In one retrospective study, administration of steroids, intravenous immunoglobulin, and plasma exchange in selected patients was most often performed to ensure that other possible and treatable diagnoses were addressed before the diagnosis of fibrocartilaginous embolism was ultimately made . The lack of available diagnostic criteria for fibrocartilaginous embolism has otherwise prevented an accurate assessment of the benefit of a specific treatment .
Generally, the prognosis is poor, with recovery encountered less frequently than with many other more common types of spinal cord ischemia .
Differential diagnosis
The generic clinical differential diagnosis of spinal stroke includes:
- transverse myelitis
- multiple sclerosis
- neuromyelitis optica
- thromboembolism
- aortic or anterior spinal artery dissection
- sickle cell disease
- vasculitis
- acute disseminated encephalomyelopathy
- arteriovenous malformations
- Guillain-Barre syndrome
- systemic lupus erythematosus
- antiphospholipid antibody syndrome
- disc prolapse or herniation
- neoplasm
Siehe auch:


 Assoziationen und Differentialdiagnosen zu FCE:
Assoziationen und Differentialdiagnosen zu FCE: