Acute spinal cord ischemia syndrome










Acute spinal cord ischemia syndrome is uncommon, but usually presents with profound neurological signs and symptoms, and the prognosis is poor.
Epidemiology
Acute spinal cord ischemia syndrome represents only 5-8% of acute myelopathies and <1% of all strokes . The demographic of affected individuals will reflect the underlying cause, although generally, two peaks are present with different etiologies. In childhood, most cases are due to trauma or cardiac malformations . In contrast, adults tend to be affected in later life, and when a cause is usually identified the result of atherosclerosis, and related complications (e.g. thoracoabdominal aortic aneurysm, thromboembolism) .
Clinical presentation
The majority of patients developed symptoms quickly, with maximal symptomatology reached within 12 hours for >50% of patients and within 72 hours for the vast majority of patients .
Initial symptoms include severe back pain (60-70%), loss of bladder control (60%) and bowel control (40%) . Perhaps a little counter-intuitive, given that the anterior cord is most commonly involved, the first symptom noticed is more frequently sensory (60%) .
Although the exact nature of neurological impairment depends on the pattern and level of involvement, generally impairment is sudden and severe with an inability to walk due to paraplegia and paraparesis with quadriplegia or tetraplegia seen in patients with higher cord lesions. Almost all patients have some sensory disturbance, and the majority of patients require urinary catheterization .
The pattern of neurological impairment can be divided into a number of separate entities, although there is much variability in the nomenclature and description of these patterns in the literature. A perhaps somewhat simplistic approach, but one that most people would agree with, divides spinal cord infarcts into two common patterns according to which spinal artery is involved :
- anterior spinal artery syndrome (most common)
- bilateral (due to single midline anterior spinal artery)
- paralysis below affected level (initially flaccid; later spastic)
- pain and temperature sensory loss
- relative sparing of proprioception and vibration (dorsal columns)
- incomplete
- anterior horn syndrome
- man-in-the-barrel syndrome if cervical
- posterior spinal artery syndrome
- usually unilateral (due to paired posterior spinal arteries)
- complete sensory loss at the level of injury
- proprioception and vibration loss below level
- minimal, typically transient, motor symptoms
There are a number of less common presentations, which vary widely in terminology, including :
- central spinal cord infarct (often the result of severe hypotension)
- sulcal artery syndrome (resulting in a partial Brown-Séquard syndrome)
- complete transverse spinal cord infarction (aka transverse medullary infarction)
Pathology
Etiology
Overall causes include :
- idiopathic (most common)
- atherosclerosis (~33%)
- aortic pathology
- aortic aneurysm
- aortic thrombosis
- aortic dissection
- aortic surgery/intervention
- vertebral artery dissection/occlusion
- atherosclerosis of vessels directly supplying the cord
- aortic pathology
- trauma, e.g. stabbing
- other rarer reported causes
- cardiac embolism
- fibrocartilaginous embolism
- Caisson disease: decompression sickness from scuba diving
- coagulopathy and hematological disorders (e.g. sickle cell disease)
- spinal arteriovenous malformations
- systemic hypotension
- epidural anesthesia
- radiation-induced vasculopathy
- vasculitis including cocaine
- sympathectomy
- gastrectomy
- esophagectomy
It is worth noting that whether chronic degenerative change of the cord, with osteophytes or disc protrusions compressing the cord, is an underlying cause of acute spinal cord ischemia is controversial .
Radiographic features
MRI is the gold standard in imaging the spinal cord and should be obtained in all patients with suspected cord infarction, not only to confirm the diagnosis but perhaps more importantly to exclude other more readily treated causes of cord impairment (e.g. compression).
MRI
The hallmark of spinal cord infarction is the presence of abnormal T2 signal within the cord, the pattern of which will depend on the territory.
Diffusion-weighted imaging is challenging in the spine, largely due to physiological CSF flow induced artifact, but can show restricted diffusion, is being increasingly used .
In the acute phase, the cord can also appear expanded due to edema.
Anterior spinal artery
Involvement of the anterior spinal artery represents the majority of cases, and the anterior and central portion of the cord are involved, most frequently bilaterally. In many instances, the anterior horn cells are primarily involved and demonstrate prominent high T2 signal resulting in pencil-like hyperintensities extending over a number of levels. On axial imaging, this appears as two bright dots, the so-called owl eye appearance .
Central involvement can be more extensive than this, involving not only the grey matter but also the central white matter, sparing only a thin rim of surrounding peripheral white matter .
In some instances, the adjacent vertebral body demonstrates infarction, although this is not a common finding .
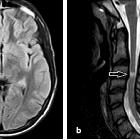
Posterior spinal artery
Usually, involvement of the posterior spinal arteries is unilateral (as posterior spinal arteries are paired) and are usually confined to the dorsal columns .
Treatment and prognosis
Not surprisingly, the degree of involvement of the cord and degree of swelling herald a poor prognosis, with many patients not being able to walk and requiring long-term urinary catheterization.
Patients who have intact proprioceptive sensation, implying spared dorsal columns, have a better prognosis, as do those with smaller infarcts (e.g. those with owl eye appearance) . Even better prognosis can be expected in patients with single sulcal artery occlusion (sulcal artery syndrome).
In one study, of patients who survived and were able to be followed up ~50% were eventually able to walk independently, 30% were able to do so with walking aids, and 20% remained wheelchair bound .
Similar outcomes were found for urinary continence, with ~50% having regained normal function, 30% having intermittent incontinence, and 20% requiring persistent catheterization .
Siehe auch:
- Transverse Myelitis
- Encephalomyelitis disseminata
- Ventriculus terminalis
- spinales Hämangioblastom
- central cord syndrome
- Brown-Séquard-Syndrom
- intramedulläre spinale Tumoren
- Adamkiewicz-Arterie
- Arteria-spinalis-anterior-Syndrom
- Akute disseminierte Enzephalomyelitis
- anterior cord syndrome
- Blutversorgung Rückenmark
- HIV myelitis
- CMV myelitis
- hämorrhagischer spinaler Infarkt
- Sarkoidose Rückenmark
- systemic lupus erythematosus of myelon
und weiter:


 Assoziationen und Differentialdiagnosen zu Spinal cord infarctions:
Assoziationen und Differentialdiagnosen zu Spinal cord infarctions: