intestinale Invagination

























intestinale Invagination
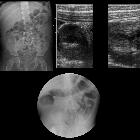
Invagination Radiopaedia • CC-by-nc-sa 3.0 • de
Intussusception occurs when one segment of bowel is pulled into itself or a neighboring loop of the bowel by peristalsis. It is an important cause of an acute abdomen in children and merits timely ultrasound examination and reduction to preclude significant sequelae including bowel necrosis. When occurring in the adult population, intussusception is usually caused by a focal lesion acting as a lead point.
Epidemiology
The vast majority of intussusceptions occur in children (95%), usually after the first three months of life .
Clinical presentation
While the classic triad of intermittent abdominal pain, vomiting, and right upper quadrant mass, plus occult or gross blood on rectal examination has great positive predictive value for intussusception in children , these findings are seen in less than 20% of intussusception cases . Approximately 15% (range 13-22%) of patients with intussusception do not even present with abdominal pain . Classic physical exam findings include an oblong palpable mass in the right upper quadrant described as "sausage-like" with a paucity of palpable bowel in the right lower quadrant .
Pathology
A proximal part of the bowel is pulled into the distal lumen and propulsed forwards as if it were a bolus of food. The prolapsing part of the bowel is described as the intussusceptum while the distal segment of bowel receiving the intussusceptum is described as the intussuscipiens. As the mesentery is incorporated into the intussusception, venous return is compromised resulting in edema and further restriction to blood flow. Eventually, arterial supply to the bowel is interrupted and ischemia and necrosis ensue.
Etiology
In children, a lead point is not identified in 90% of cases, and this is most frequently thought to relate to hypertrophic lymphoid tissue following an infection. This potentially explains the relative rarity of the condition in the first three months of life, when passive immunity is still paramount.
In infants and adults, a lead point is more frequently identified with up to 90% of adult cases having a lead point (which is usually malignant in the large bowel and benign in the small bowel ).
Lead points are numerous and include :
- gastrointestinal malignancy (most common cause in adults, accounting for 65% of cases )
- colorectal carcinoma (most common)
- metastases, e.g. malignant melanoma, breast cancer, lung cancer
- small bowel lymphoma/Burkitt lymphoma
- benign neoplasms
- gastrointestinal stromal tumor (GIST)
- intestinal polyps
- intestinal lipoma
- polypoid hemangioma
- appendiceal mucocele
- congenital
- inflammatory
- periappendicitis
- trauma
- mural hematoma
Radiographic features
Intussusception can occur essentially anywhere. In adults, no pattern of distribution is present as such as in the vast majority of cases a lead point lesion is present, and thus the location will depend on the location of that lesion. In children there is a strong predilection for the ileocolic region:
- ileocolic: most common (75-95%), presumably due to the abundance of lymphoid tissue related to the terminal ileum and the anatomy of the ileocecal region
- ileoileocolic: second most common
- ileoileal and colocolic: uncommon
- gastric intussusception: rare, but documented
Plain radiograph
Abdominal x-rays may demonstrate an elongated soft tissue mass (typically in the upper right quadrant in children) with bowel obstruction (and therefore air-fluid levels and bowel dilation) proximal to it. There may be an absence of gas in the distal collapsed bowel.
Fluoroscopy
A contrast enema remains the gold standard, demonstrating the intussusception as an occluding mass prolapsing into the lumen, giving the "coiled spring” appearance (barium in the lumen of the intussusceptum and in the intraluminal space). The main absolute contraindication for an enema is a perforation, which needs to be treated surgically.
Ultrasound
Ultrasonography has a false-negative rate approaching zero and is a reliable screening tool for children at low risk for intussusception . Children with classic findings of intussusception, however, need to be investigated with an enema, which is both diagnostic (the gold standard in the diagnosis of intussusception) and therapeutic.
Ultrasound signs include:
- target sign (also known as the doughnut sign)
- pseudokidney sign
- crescent in a doughnut sign
Some ultrasound features favor ileocolic over small bowel intussusception :
- presence of a hyperechoic core, representing mesenteric fat
- diameter of the fatty core exceeding that of the outer wall
- larger anteroposterior diameter (mean 2.6 cm vs. 1.4 cm)
- diameter over 2 cm strongly argues in favor of ileocolic
- thicker outer hypoechoic wall (mean 0.6 cm vs 0.4 cm)
- lymph nodes inside the intussusception
Small bowel intussusception has a predilection for the paraumbilical to left upper/lower quadrants of the abdomen . While typically transient, surgical management may be required if spontaneous reduction is unlikely to occur. Sonographic features which are considered more consistent with an uncomplicated clinical course include:
- outer diameter < 2.5 cm
- preserved bowel wall motility
- no identifiable lead point
- lesion length < 3 cm
CT
CT has become the modality of choice for assessment of acute abdomen in adults, and thus most frequently images intussusception. Also, short length transient intussusception is a frequent incidental finding.
The appearance of intussusception on CT is characteristic and depends on the imaging plane and where along the bowel the images are obtained.
Best known is the so-called bowel-within-bowel configuration, in which the layers of the bowel are duplicated forming concentric rings (CT equivalent of the ultrasonographic target sign) when imaged at right angles to the lumen, and a soft tissue sausage when imaged longitudinally .
At the proximal end of the intussusception, there will be two concentric enhancing/hyperdense rings, formed by the inner bowel and the folded edge of the outer bowel. As one images further along the intussusception the mesentery (fat and vessels) will form a crescent of tissue around the compressed innermost lumen, surrounded by the two layers of the outer enveloping bowel. Even further distally the lead point (if present) will be visualized .
Treatment and prognosis
In children, intussusception reduction can be achieved without recourse to surgery in most cases. Using a water-soluble medium or air introduced via a rectal catheter, retrograde pressure can be exerted to reduce the intussusception. If symptoms have been protracted, rectal blood is present; there are signs of peritonitis or enema reduction is unsuccessful then surgical intervention is usually required. With no surgical treatment, there can be recurrence rates of up to 30%.
In adults, a laparotomy is usually required, especially as in most cases a lead point requiring treatment is present.
Differential diagnosis
On imaging the appearances on ultrasound and CT are characteristic. The main differential is that of transient intussusception, which is an incidental finding requiring no treatment or follow-up.
Other conditions to be considered in adults include:
- primary bowel tumor
- metastases and lymphoma
- intestinal lipoma (without intussusception)
- Meckel diverticulum
- gallstone ileus (cholesterol stones can have a layered appearance with fat density)
- endometrial implant
Siehe auch:
- Gallensteinileus
- Invagination
- ileokolische Invagination
- Lipome des Gastrointestinaltraktes
- Peutz-Jeghers-Syndrom
- Dünndarminvagination
- Target-Zeichen bei Invagination
- bull's eye sign
- Kolonlipom
- transiente Invagination
- Koloninvagination
- ileokolische Invagination beim Erwachsenen
- Invagination der Appendix
- pseudokidney of intussusception
- Invagination bei Kindern
- Dünndarmileus durch Invagination
- Devagination
- idiopathische Koloninvagination
- retrograde jejunogastrale Invagination
und weiter:
- intermittent intussusception in Henoch-Scholein Purpura
- crescent in a doughnut sign
- intussusception on ultrasound
- gastrointestinale Lipomatose
- appendiceal intussusception
- intestinal malrotation and intussusception
- complicated Peutz Jeghers syndrome
- ileocolische Invagination, pneumatische Devagination
- Peutz-Jeghers syndrome complicated by intussusception
- chronic colocolic intussusception
- fettige Infiltration der Magenwand
- multiple small bowel lipomas with intussusception
- Invagination durch einen inflammatorischen fibroiden Polypen


 Assoziationen und Differentialdiagnosen zu intestinale Invagination:
Assoziationen und Differentialdiagnosen zu intestinale Invagination: 





