Mediastinal masses

Isolated
middle mediastinal mass associated with immunoglobulin G4-related disease. Preoperative imaging. a Chest X-ray showed an abnormal mass in the left mediastinum (yellow arrowheads). b Enhanced computed tomography of lung field (yellow arrowheads). c Enhanced computed tomography of mediastinal field; the left mediastinal mass was a homogenous round-shaped 3.8 × 2.4 cm in diameter (yellow arrowheads)

A diagnostic
approach to the mediastinal masses. A cystic lymphangioma (also referred to as hygroma) in a 47-year-old woman with retroperitoneal disease. A posterior mediastinal mass with a homogeneous fluid-attenuation is identified on CT (white arrow) and on posteroanterior chest radiograph as a mass disrupting left paraspinal line inferiorly (black arrows)

A diagnostic
approach to the mediastinal masses. A well-marginated mass with a homogeneous attenuation, usually in the range of water attenuation (0–20 HU) and without an enhancement of the wall or infiltrative appearance are the typical features of benign mediastinal cysts. Probably thymic cystic (a) and pericardial cyst (b)

A diagnostic
approach to the mediastinal masses. Oblique-coronal multiplanar reconstruction of contrast-enhanced CT scan of a 33-year-old woman with a descending necrotising mediastinitis. Hypodense para-aortic areas correspond with fluid-collections (arrows) that extend to the retroperitoneum. Pleural effusion in the fissure is also be seen (open arrow). Note the visceral space involvement (arrowhead)

A diagnostic
approach to the mediastinal masses. Bronchogenic cyst in a 37-year-old man. a Non-contrast-enhanced CT scan shows a homogeneous anterior mediastinal mass with smooth contours and oval shape (arrow). The mass is isodense relative to chest wall muscle. b T2-weighted MR image shows the same mass (arrow) with markedly high signal intensity. c Although its localisation, a bronchogenic cyst was confirmed by histological examination after surgical resection

A diagnostic
approach to the mediastinal masses. a Lateral chest radiograph of a 58-year-old smoker man allergic to iodine shows a well-defined mass (*) in the cardiophrenic space and a nodular lung opacity (open arrow) in the lower lung parenchyma. b, c Non-contrast-enhanced CT scan confirms the presence of a fluid-attenuation mass (*) in the right cardiophrenic angle (pericardial cyst) and demonstrates a suspicious lung opacity (open arrows) in the right lower lobe of the lung (squamous-cell carcinoma)

A diagnostic
approach to the mediastinal masses. Thymic lymphoid hyperplasia in a 41-year-old woman with clinical diagnosis of myasthenia gravis. Non-contrast-enhanced CT scan shows an enlarged thymic gland (arrows) without mass effect on adjacent structures

A diagnostic
approach to the mediastinal masses. Congenital thymic cyst in a 47-year-old man. Contrast-enhanced CT scan demonstrates a unilocular unenhanced lesion in the anterior mediastinum which shows a homogeneous fluid-attenuation (arrow)

A diagnostic
approach to the mediastinal masses. Acquired thymic cyst in a 43-year-old man. a Contrast-enhanced CT scan shows a well-defined water-attenuation multiloculated mass (*) in the anterior mediastinum. b Sagittal T2-weighted MR sequence demonstrates a multiloculated mass with typical high signal intensitiy and fine internal septa within (arrow)

A diagnostic
approach to the mediastinal masses. Pancreatic pseudocyst in a 52-year-old man with a recurrent pancreatitis history. Axial (a, b) and oblique-sagittal multiplanar reconstruction (c) CT scan show a thin-walled peri-oesophageal fluid-lesion (white open arrows) that comunicates with an intrapancreatic fluid-collection (black open arrows) through oesophageal hiatus by a duct fistula (white arrows)

A diagnostic
approach to the mediastinal masses. Different masses arising from the digestive tract. a Oesophageal stenosis after Nissen fundoplication (arrow). b Posterior mediastinal mass (arrow) in relation with squamous-cell carcinoma of the oesophagus. c Oesophageal diverticulum (arrow) in a patient with oesophageal achalasia. Note the thickened oesophagus. d Hiatal hernia is a frequent incidental finding with or without air or air-fluid level (open arrow). * Pleural effusion

A diagnostic
approach to the mediastinal masses. Mediastinal goitres. a Coronal multiplanar reconstruction CT scan demonstrates an anterior mediastinal mass (*) arising from the thyroid more superiorly. Note the cystic degeneration within goitre (open arrow). b Non-contrast-enhanced CT scan shows a unilateral mediastinal goitre with peripheral areas of calcification (open arrow). c Photograph of the resected surgical specimen shows a lobulated and heterogeneous appearance of the mass. d Contrast-enhanced CT scan shows a well marginated posterior mediastinal goitre (*) with marked contrast enhancement

A diagnostic
approach to the mediastinal masses. a Heterotopic mediastinal goitre. Sagittal contrast-enhanced CT scan demonstrates a well-defined mass (arrow) located in the retrosternal space which shows an intense and heterogeneous contrast enhancement due to the presence of cystic areas (*). No connection to the thyroid gland from the neck. b Anaplastic thyroid carcinoma in a 64-year-old woman with respiratory failure. Contrast-enhanced CT scan shows an anterior mediastinal soft tissue mass (*) which surrounds great vessels and oesophagus and compresses trachea. Note the extension to the suprasternal fossa (open arrow)

A diagnostic
approach to the mediastinal masses. a Contrast-enhanced CT scan of a man who had suffered a traffic accident. An infiltrative mediastinal haematoma is identified with subtle areas of high CT-attenuation values (arrow). Bilateral pleural effusion (*) and a sternum fracture (open arrow) are also observed. b Iatrogenic mediastinal haematoma (arrow) in a 64-year-old man secondary to bronchoscopy with transtracheal biopsy. Note the high attenuation value of the lesion compared with muscular tissue

Mediastinum
• Mediastinal anatomy - Gray's anatomy illustration - Ganzer Fall bei Radiopaedia
Mediastinum
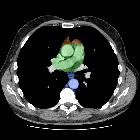
• Mediastinal compartments: annotated CT - Ganzer Fall bei Radiopaedia

Multinodular
goiter • Superior mediastinal mass - multinodular goiter - Ganzer Fall bei Radiopaedia

Mediastinal
mass • Pericardial cyst - Ganzer Fall bei Radiopaedia

A diagnostic
approach to the mediastinal masses. Thymolipoma in a 47-year-old asymptomatic man. Axial and coronal multiplanar reconstruction of non-contrast-enhanced CT scan show a large and well-defined mass (arrows) that has extensive fat content and contains small amounts of thin fibrous septa

A diagnostic
approach to the mediastinal masses. a Contrast-enhanced CT scan shows a right-sided aortic arch (arrow) in an asymptomatic man with an absence of the aortic knuckle on the left. b Contrast-enhanced CT scan demonstrates a soft tissue posterior mediastinal mass (*) in a 66-year-old woman with multiple myeloma diagnosis. Note the mass effect to the descending aorta and left auricula by the mass and the bilateral pleural effusion (open arrows)

A diagnostic
approach to the mediastinal masses. Chest imaging shows well the highly heterogeneous contents of mediastinal teratomas. a Mature cystic teratoma in a 40-year-old man. Contrast-enhanced CT scan shows a heterogeneous anterior mediastinal mass with areas of fat (open arrow), calcification (arrow) and fluid attenuation (*). Posterior displacement of mediastinal structures is also be seen. b Photograph of the surgical specimen. c Contrast-enhanced CT scan of an asymptomatic 24-year-old woman demonstrates a well-defined uniloculated mass located in prevascular space which shows a cystic changes within (*). Non foci of calcification were identified. d The mass was surgically removed and pathological examination confirmed a benign teratoma

A diagnostic
approach to the mediastinal masses. a, b Stage II thymoma (WHO type B1) in a 33-year-old woman who presented with myasthenia gravis. Frontal chest radiograph shows a hilum overlay sign (arrow) of a suggestive anterior mediastinal mass. Contrast-enhanced CT scan confirms the presence of a low-heterogeneous anterior mediastinal mass (arrow). Note the indentation of the arterial trunk pulmonary by the mass. c, d Stage III thymoma (WHO type B2) in a 54-year-old woman. Frontal chest radiograph reveals a lobulated mediastinal mass (arrow) on the right side. Contrast-enhanced CT scan demonstrates an enhanced anterior mediastinal mass (arrow) with infiltration of surrounding fat (open arrow)

A diagnostic
approach to the mediastinal masses. Stage IVa thymoma (WHO type B2) in a 46-year-old man. a Contrast-enhanced CT scan reveals an anterior mediastinal mass (arrows) with irregular contours, homogeneous enhancement and peripheral and central calcification as well as a pleural nodule (open arrow). b On an axial FDG-positron emission tomography (PET) image, the pleural nodule is FDG avid, confirming a drop metastasis. c Image during the surgical resection. d Photomicrograph (haematoxylin-eosin stain) of tissue from the lesion shows roughly equal numbers of epithelial cells (white arrow) and lymphocytes (black arrow) corresponding thymoma WHO type B2

A diagnostic
approach to the mediastinal masses. Axial (a) and coronal multiplanar reconstruction (b) of a non-contrast-enhanced CT scan of a 57-year-old man allergic to iodine with a thymoma. A solid lobulated thymic mass (*) with clumps of calcifications within (arrowhead) is identified. Note the absence of a fat plane between the tumour and the aorta (open arrow). d Coronal T2-weighted MR image shows a typical signal hyperintensity of the tumour lesion (*). c Axial contrast-enhanced fat-suppressed T1-weighted MR image reveals a homogeneously enhanced solid tumour (*) which arises from the thymus. Although MRI demonstrates the presence of fat cleavage plane between ascending aorta and the tumour, a thymoma (WHO type A) with microscopic transcapsular invasion (Masaoka stage II) was confirmed after surgical resection

A diagnostic
approach to the mediastinal masses. A 28-year-old man with Hodgkin lymphoma. Frontal chest radiograph and contrast-enhanced CT scan show a homogeneous soft tissue mass at the level of the subcarina (arrows). An aortopulmonary window lymphadenopathy can be detected on CT scan (open arrow). The right paratracheal stripe is not seen on frontal chest radiograph, having been most probably obliterated by a right paratracheal lymphadenopathy (arrowhead). * Carina

A diagnostic
approach to the mediastinal masses. Nodular sclerosis Hodgkin lymphoma in a 44-year-old woman. Frontal chest radiograph shows a large, well-defined mediastinal mass with increased density (arrow). Contrast-enhanced CT scan shows a bulky soft tissue mass (arrows) with homogeneous CT-attenuation value occupying prevascular space. Note the left internal mammarian artery completely surrounded by the lesion. Photomicrograph reveals numerous neoplastic lacunar cells (arrows) in a background of small lymphocytes, histiocytes and eosinophils, which supports the diagnosis of nodular sclerosis type Hodgkin lymphoma

A diagnostic
approach to the mediastinal masses. Axial T1-weighted MR image of a 16-year-old man with a solid, large mass (arrows) in the anterior and superior mediastinum. Supra-aortic trunks are almost completely surrounded by the lesion and trachea (T) is displaced to the contralateral side by the lesion. Pathological analysis demonstrated a T-cell lymphoblastic lymphoma

A diagnostic
approach to the mediastinal masses. Primary mediastinal diffuse large B-cell lymphoma in a 19-year-old man. Contrast-enhanced CT scan shows a bulky soft tissue mass in the anterior mediastinum (arrowsin a), which shows heterogeneous CT-attenuation values with cystic changes within (*). Pericardial effusion is also observed (open arrow in b)

A diagnostic
approach to the mediastinal masses. A 19-year-old man with seminoma. Contrast-enhanced axial CT scan demonstrates a large mass in the right side of the mediastinum with an obvious mass effect on great vessels and heart. The mass shows heterogeneous CT-attenuation values probably secondary to haemorrhage and coagulation necrosis. Note also a right pleural effusion (arrowhead) and multiple lung metastasis (arrows)

A diagnostic
approach to the mediastinal masses. Non-seminomatous malignant germ cell tumour of the anterior mediastinum in a 25-year-old man with chest pain and high serum level of α-fetoprotein at admission (25.396 ng/ml). Frontal chest radiograph shows a central mass (*). The descending aorta is clearly seen (arrows), indicating that the mass is not within the posterior mediastinum. Multiple nodules in bilateral pulmonary field are also observed. A contrast-enhanced CT scan confirms a mass of low attenuation (*) in the anterior mediastinum that compresses the pulmonary artery. Bilateral lung metastasis (arrowheads) and hilar and subcarinal lymphadenopathy is identified (open arrows)

A diagnostic
approach to the mediastinal masses. Duplication cyst in a 42-year-old asymptomatic man. a Contrast-enhanced CT scan shows a round well marginated mass (arrow) adjacent to the oesophagus with homogeneous water-attenuation. b The lesion (arrow) presents a bright signal intensity on T2-weighted fat-suppressed MR image

A diagnostic
approach to the mediastinal masses. Peripheral nerve tumours usually show a markedly convex mass arising from the mediastinum. a Coronal multiplanar reconstruction of contrast-enhanced CT scan of an asymptomatic 59-year-old man with a mass in right superior mediastinum (arrow). Histological examination confirmed a schwannoma arising from the phrenic nerve. b Schwannoma in a 77-year-old woman. Non-contrast-enhanced CT scan shows a well-defined and homogeneous paravertebral mass (*)

A diagnostic
approach to the mediastinal masses. Neuroblastoma in a 20-year-old man. Axial (a) and coronal (b) T2-weighted MR images, and sagittal (c) contrast-enhanced T1-weighted MR image demonstrate an expansive and heterogeneous mass in the left paravertebral space which shows cystic degeneration within (*) as well as an intensive enhancement (in c). Note the spinal involvement (arrowhead in b)

A diagnostic
approach to the mediastinal masses. Aortopulmonary paraganglioma in a 52-year-old woman. a Enhanced-CT scan shows a markedly enhancing lesion (arrow) located adjacent of the arch of aorta. b Image during the surgical remove of the lesion. Paraganglioma (white arrow); descending aorta (black arrow); vagus nervus (open arrow). c Photomicrograph demonstrated a trabecular pattern of growth and scattered ganglion-like cells surrounded by fibrovascular septa (arrows)

A diagnostic
approach to the mediastinal masses. Parathyroid adenoma in a 66-year-old man with hypercalcaemia, hypophosphataemia and elevated PTH values. Tc-99m MIBI scan shows a focus of hyperactivity (black arrow) adjacent to the lower pole of left thryoid lobule. Enhanced-CT scan shows a superior mediastinal enhanced mass (white arrow)

A diagnostic
approach to the mediastinal masses. Idiopathic fibrosing mediastinitis in a 64-year-old man. a Coronal multiplanar reconstruction and axial b constrast-enhanced CT scan show an infiltrating soft tissue mass (white arrows) in mediastinum encasing major vessels. Punctate calcifications are observed (black arrows) as well as an elevation of the right hemidiaphragm (open arrow) secondary to the phrenic nerve involvement

A diagnostic
approach to the mediastinal masses. CT is the imaging modality of choice for evaluating staging thymoma. Stage IVa thymoma (WHO type B3) in a 69-year-old woman. a, b Contrast-enhanced CT scan shows a well-circumscribed, flattened soft tissue lesion in the anterior mediastinum with calcification (arrow). Note the lobulated contour of the mass and the loss of the fat plane between the mass and the aorta. Pleural seeding is identified as an enhancing pleura-based nodule (open arrow). c Irregular border between the mediastinal mass and the lung parenchyma (arrowhead) is observed as a sign of locally advanced disease. Note the cellular bronchiolitis in the left lower lobe

A diagnostic
approach to the mediastinal masses. a–c Thymic hyperplasia in a 43-year-old woman (arrows). a Non-contrast-enhanced CT scan reveals a lobulated lesion with smooth margins in anterior mediastinum. b Lesion appears slightly hyperintense on in-phase gradient-echo T1-weighted MR image. c Opposed-phase gradient-echo T1-weighted MR image shows decreased signal intensity within the lesion, confirming presence of fat. d–f Stage II thymoma (WHO type B2) in a 62-year-old woman (arrows). d Non-contrast-enhanced CT scan shows an anterior mediastinal soft tissue mass. e The lesion shows an intermediate signal intensity on in-phase gradient-echo T1-weighted MR image. f There is no substantial decrease in signal intensity relative to in-phase MR image on opposed-phase sequence

A diagnostic
approach to the mediastinal masses. Conventional radiograph can provide information pertaining to the size, anatomical location and density of a central mass. Right: Frontal chest radiograph shows a sharply defined area of increased opacity with a loss of the cardiac silhouette at the border of the right side of the heart (*). Contrast-enhanced CT scan reveals a thin-walled water-attenuation lesion (*) in the right cardiophrenic angle (pericardial cyst). Middle: Lateral chest radiograph and contrast-enhanced CT scan show a unilocular, well-defined and homogeneously hypodense mass in the anterior mediastinum with peripheral calcification (open arrows) (thymic cyst). Left: Chest radiograph shows the aortopulmonary window with an abnormal convex border (arrow). Contrast-enhanced CT scan demonstrates a multilobulated mass in the anterior mediastinum (arrow), which accounts for the distortion of the AP window (nodular sclerosis Hodgkin disease)

Mediastinal
mass • Posterior mediastinal mass - Ganzer Fall bei Radiopaedia
Mediastinal masses may be caused by a wide variety of neoplastic and non-neoplastic pathologies. It is helpful to identify the location of the mass since this significantly reduces the breadth of the differential diagnosis.
There are four conceptual compartments of the mediastinum which are dictated by their relationships to the thoracic plane and pericardium:
- superior mediastinum: above the thoracic plane
- inferior mediastinum: below the thoracic plane
- anterior mediastinal mass: anterior to the pericardium
- middle mediastinal mass: within the pericardium
- posterior mediastinal mass: posterior to the pericardium
Siehe auch:
- Mediastinum
- Bronchogene Zyste
- Azygoskontinuität
- Perikard
- Tumoren des vorderen oberen Mediastinums
- Morbus Castleman
- mediastinales Teratom
- Tumoren des hinteren Mediastinums
- thorakales Aortenaneurysma
- Thymuslipom
- Struma
- Metastasen bei Mammakarzinom
- Aortenaneurysma
- invasives Thymom
- mediastinale Lymphadenopathie
- Lymphadenopathie
- vorderes Mediastinum
- mediastinale Sarkome
- Gefäßmalformation Mediastinum
- IgG4-assoziierte Erkrankung des Mediastinums
- paraspinal abscess
- Tumoren des oberen Mediastinums
- mediastinales Lymphangiom
und weiter:


 Assoziationen und Differentialdiagnosen zu mediastinale Raumforderungen:
Assoziationen und Differentialdiagnosen zu mediastinale Raumforderungen: