Bronchogene Zyste





















Bronchogenic cysts are congenital malformations of the bronchial tree (a type of bronchopulmonary foregut malformation). They can present as a mediastinal mass that may enlarge and cause local compression. It is also considered the commonest of foregut duplication cysts.
Epidemiology
Bronchogenic cysts are rare congenital lesions accounting for only 5-10% of pediatric mediastinal masses . The incidence of mediastinal cysts is equal between the sexes whereas intrapulmonary cysts are reported to have a male predilection .
Clinical presentation
In many instances, bronchogenic cysts are asymptomatic and are found incidentally when the chest is imaged . When large, mass effect may result in bronchial obstruction leading to air trapping and respiratory distress. An alternative presentation may occur when the cyst becomes infected.
Pathology
Bronchogenic cysts form as a result of abnormal budding of the bronchial tree during embryogenesis (between 4-6 weeks) , and as such, they are lined by secretory respiratory epithelium (cuboid or columnar ciliated epithelium) . The wall is made up of tissues similar to that of the normal bronchial tree, including cartilage, elastic tissues, mucous glands, and smooth muscle .
They do not usually communicate with the bronchial tree and are therefore typically not air-filled. Rather, they contain fluid (water), variable amounts of proteinaceous material, blood products, and calcium oxalate . It is the latter three components that result in increased attenuation mimicking solid lesions. They are rarely multiple.
Distribution
They can occur in the mediastinum or be intrapulmonary. The most common location is the middle mediastinum (65-90%). The distribution of locations can be quite varied:
- mediastinal (~70%)
- usually does not communicate with the tracheobronchial tree
- subcarinal, right paratracheal and hilar locations most common
- approximate incidence includes
- carinal area: ~50%
- paratracheal area: ~20%
- oropharyngeal wall: ~15%
- retrocardiac area: ~10%
- parenchymal (intrapulmonary)
- typically perihilar
- predilection for lower lobes
- other uncommon locations
- neck
- cutaneous
- pericardium
- extending across the diaphragm and appearing dumb-bell shaped
- retroperitoneal : tend to be in a subdiaphragmatic or peripancreatic distribution, usually to the left of the midline
Radiographic features
Although bronchogenic cysts are usually fluid-filled, occasionally a communication may develop following infection or intervention, resulting in an air-filled cystic structure +/- an air-fluid level .
Plain radiograph
The cysts usually appear as soft-tissue density rounded structures, sometimes with compression of surrounding structures. Occasionally such compression can lead to air-trapping and a hyperlucent hemithorax . As the cysts may contain calcium oxalate, dependent layering of calcific density material (milk of calcium) may on occasion be seen .
CT
Typically appear as well-circumscribed spherical or ovoid masses of variable attenuation with variable fluid composition explaining the different CT attenuations observed.
Approximately 50% are fluid density (0-20 HU), however, a significant proportion is of soft tissue density (>30 HU) or even hyperattenuating to surrounding mediastinal soft tissues . The degree of CT attenuation often depends on the amount of internal proteinaceous content . CT is better able to detect calcium oxalate (milk of calcium) layering dependently .
There is no solid contrast enhancement.
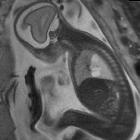
MRI
Sometimes performed for confirmation, especially with atypical cases. Mostly homogeneous .
- T1:
- variable signal intensity, from low (similar to fluid) to high (due to protein content)
- fluid-fluid level has also been reported, attributed to the layering of variable fluid content
- T2:
- usually high signal intensity due to fluid content
Treatment and prognosis
The choice of treatment is somewhat controversial. Some authors advocate surgical excision of all cysts given their tendency to become infected or rarely, to undergo malignant transformation . Increasingly, these lesions are treated with transbronchial or percutaneous aspiration under CT guidance to both confirm the diagnosis and to treat them. Small lesions can be followed, however, they do have a tendency to increase in size over time, sometimes rapidly .
Complications
- fistula formation with the bronchial tree
- ulceration of the cyst wall
- secondary bronchial atresia
- superimposed infection
- hemorrhage
- malignant transformation is very rare (0.7% risk ), but reported, with primaries including :
- rhabdomyosarcoma
- pleuropulmonary blastoma
- anaplastic carcinoma
- leiomyosarcoma
- adenocarcinoma
Differential diagnosis
General imaging differential considerations for uncomplicated cysts include:
- congenital cysts and malformations
- pericardial cyst
- cystic hygroma and lymphangioma
- neurenteric cyst
- anterior or lateral meningocoele
- esophageal duplication cyst
- thyroid colloid cyst
- thymic cyst
- intrathoracic pancreatic pseudocyst (for retroperitoneal bronchogenic cysts or for pancreatic pseudocysts that extend intra thoracically through the aortic hiatus or esophageal hiatus)
If complicated, e.g. with infection or hemorrhage, also consider:
- abscess(es)
- enlarged lymph nodes, especially if centrally necrotic
- pulmonary masses
- focal hematoma: different clinical context
See also
Siehe auch:
- Lungenkarzinom
- Lungensequester
- Pankreaspseudozyste
- Perikardzyste
- kongenitale pulmonale Atemwegsmalformation (CPAM)
- Meningozele
- Lymphangiom
- Duplikationszyste des Ösophagus
- neuroenterische Zyste
- zystisches Lymphangiom
- zervikale bronchogene Zyste
- Thymuszyste
- pulmonary pseudotumour
- kindliche Lungenläsionen
- Ösophagusduplikatur versus bronchogene Zyste
und weiter:
- Kavernöse Lungenläsionen
- Lungenzysten
- cystic mediastinal masses
- mediastinales Teratom
- mediastinale Raumforderungen
- Mukoidimpaktion
- pulmonary cavity (mnemonic)
- Duplikationszyste des Vorderdarms
- Rundpneumonie
- Pleuro-pulmonales Blastom
- Lungensequester extralobulär
- zystische Lungenläsionen bei Kindern
- cytic lung lesions - paediatric
- Bronchozele
- Migrating pericardial cyst
- bronchopulmonale Vordarmmalformation
- mediastinal bronchogenic cyst
- MacLeod syndrome and bronchogenic cyst
- Acute Respiratory Distress Syndrome neonatal
- deviation of the azygoesophageal recess line
- Ösophagusduplikatur
- intrapulmonale bronchogene Zyste mit Dyspnoe
- intrapulmonale Zyste mit einer hindurchziehenden dilatierten Pulmonalvene


 Assoziationen und Differentialdiagnosen zu Bronchogene Zyste:
Assoziationen und Differentialdiagnosen zu Bronchogene Zyste: