Lymphangiom















Lymphatic malformations are benign lesions of vascular origin that show lymphatic differentiation. Specifically, they are vascular malformations and not vascular tumors as per the 2018 ISSVA classification of vascular anomalies .
This article focuses on the general features of lymphatic malformations. For a specific discussion in other locations, please refer to:
- head and neck: cystic hygroma (cystic or nuchal lymphangioma)
- hepatic lymphangioma
- splenic lymphangioma
- pancreatic lymphangioma
- renal lymphangioma
- retroperitoneal lymphatic malformation
Terminology
These malformations were formerly called lymphangiomas. This expression is out-of-date according to the 2018 ISSVA classification .
Epidemiology
They can present at any age but most often occur in the pediatric population (~90% in those less than 2 years old ). The worldwide incidence of lymphangiomas is 1:6000-16000 live births. Males and females are equally affected.
Clinical presentation
Generally, the presentation may be with symptoms related to local mass effect and/or hemorrhage.
For example, a lymphatic malformation within the orbit may present with progressive proptosis with acute deterioration in symptoms, the mass effect resulting in compressive optic neuropathy, diplopia/ocular muscle weakness, and orbital bruising.
The clinical examination may reveal soft, non-tender masses on palpation with a doughy consistency.
Pathology
Typically comprised of thin-walled cystic masses and can be classified according to the size of the cystic lesions :
- macrocystic lymphatic malformation
- previously known as cystic hygroma / cystic lymphangioma, although a term still commonly used when large in the cervical region
- mean diameter of cystic lesions >1 cm
- microcystic lymphatic malformation
- previously known as cavernous lymphangioma
- mean diameter of cystic lesions <1 cm
- mixed type lymphatic malformation: both macroscopic and microscopic features
Their wall consists of connective tissue, smooth muscle, fat, blood vessels, nerve, and/or lymphatic tissue.
Location
They can occur at almost any location:
- marked predilection in the head and neck: 95% in the neck and axillary regions
- mesentery, retroperitoneum, abdominal viscera, lung, and mediastinum: ~5%
Associations
- lymphangioleiomyomatosis
- Noonan syndrome
- Turner syndrome
- trisomies 13, 18 and 21
Radiographic features
Lymphatic malformations may cross more than one compartment. For instance, in the head and neck region, larger lesions tend to occupy more than one deep space, sandwiching between normal structures.
Ultrasound
- multilocular cystic masses
- internal septa of varying thickness
- cystic contents: usually anechoic, hyperechoic if debris, high lipid concentration, infection or hemorrhage
- wide variations exist: solid areas, or mostly solid with cystic foci
- color Doppler: +/- arterial or venous flow in the septa
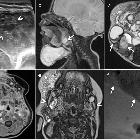
CT
Most lymphatic malformations appear homogeneous and cystic on CT, but some appear inhomogeneous because of the presence of proteinaceous, fluid, blood, or fat components within the lesion. It is rare for CT to demonstrate intrinsic septations. There is only minimal or no displacement/compression of adjacent structures.
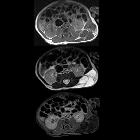
MRI
Fluid-fluid levels may be seen if complicated by hemorrhage. Signal characteristics include:
- T1: can be variable especially dependent on protein content
- T2: usually high signal
Treatment and prognosis
Surgical excision or interventional sclerotherapy (with interferon, OK-432, or bleomycin) is often necessary . Other possible treatment methods include steroid therapy, laser treatment, aspiration, radiofrequency ablation, or cautery.
Differential diagnosis
Differentials will depend on which compartment or viscera is considered. Possible imaging differential considerations include:
- hemangioma
- venous malformation: demonstrate internal blood flow and central enhancement
- other cystic neck masses
- teratoma: demonstrate fat or calcification
Siehe auch:
- Hämangiom
- Lymphangioleiomyomatose
- zystisches Lymphangiom
- oberflächliche Weichteilläsionen der Extremitäten
- Lymphangiomatose
- Lymphangiosarkom
- Lymphangiom der Orbita
- Lymphangiom mit Einblutung
- Lymphangiom der Leber
und weiter:
- Bronchogene Zyste
- intraorbitale Raumforderungen
- Splenomegalie
- cystic mediastinal masses
- Parotistumoren
- Tumoren der Speicheldrüsen
- Lymphangiom Milz
- Tumoren der Thoraxwand
- WHO Klassifikation der Weichteiltumoren
- orbital pathology
- Thymuszyste
- zystisches Lymphangiom des Mesenterium
- zervikaler Abszess
- Infantile Myofibromatose
- midline nasal region lesions
- zervikales zystisches Lymphangiom
- classification of paediatric midface anomalies
- tumours of blood vessels
- benign vascular tumours
- zystisches Lymphangiom des Rückens
- mesenteric and retroperitoneal lymphoma
- adrenal lymphangioma
- zervikale Lymphangiome
- thorakales Lymphangiom mit akuter Einblutung
- benign tumour of vascular origin
- parotid lymphangioma
- retroperitoneales Lymphangiom
- zervikale Mittellinienraumforderungen
- Makroglossie
- Erweiterung Lymphgefäße
- Lymphangiom des Fußes
- soft tissue lymphangioma
- Lymphangiom postoperativ
- Lymphangiom des Pankreas
- makrozystisches Lymphangiom
- Lymphangiom des Ösophagus
- intrapulmonale bronchogene Zyste


 Assoziationen und Differentialdiagnosen zu Lymphangiom:
Assoziationen und Differentialdiagnosen zu Lymphangiom:




