pulmonary interstitial emphysema







Pulmonary interstitial emphysema (PIE) refers to the abnormal location of gas within the pulmonary interstitium and lymphatics usually due to positive pressure ventilation. It typically results from rupture of overdistended alveoli following barotrauma in infants with respiratory distress syndrome. It may also occasionally be incidentally detected in adults.
Epidemiology
Pulmonary interstitial emphysema (PIE) is almost always associated with mechanical ventilation or continuous positive airway pressure in the first weeks of life.
Reduced lung compliance, prematurity, low birth weight, meconium aspiration syndrome and pneumonia are other risk factors.
The reported incidence of PIE amongst infants admitted to the neonatal ICU is 2-3% . The incidence rises to 20-30% among premature infants. The highest frequencies are seen in low-birth-weight infants .
Clinical presentation
Pulmonary interstitial emphysema (PIE) is typically an incidental finding on routine chest radiographs in the NICU (neonatal intensive care unit) before the onset of symptoms. If it is more extensive, it may result in compression of adjacent lung and vasculature. This can impede both ventilation and pulmonary blood flow, which can affect oxygenation, ventilation, and blood pressure. PIE may also present with air-block complications such as pneumomediastinum, pneumothorax, pneumopericardium, pneumoperitoneum, or subcutaneous emphysema.
Pathology
Pulmonary interstitial emphysema (PIE) almost always occurs during the first weeks of life in newborns on ventilatory support. Alveolar pressure increases in the setting of mechanical ventilation or continuous positive airway pressure. A combination of increased pressure and poor compliance can result in alveolar rupture with the escape of air into the adjacent interstitium and lymphatics. This interstitial air may resolve spontaneously, persist chronically or progress with further air-leak into adjacent spaces, causing pneumomediastinum, pneumothorax, pneumopericardium, pneumoperitoneum, or subcutaneous emphysema.
Overall lung volumes are increased; however, the lungs are less compliant because they are splinted at a large volume by the air within the interstitium. This may further compromise the already critically ill child. Air-block complications of PIE such as pneumomediastinum, pneumothorax and pneumopericardium can be fatal.
Location
Pulmonary interstitial emphysema (PIE) may be focal, affecting one lobe/lung or may be diffuse and bilateral. It has no predilection for any particular lobe.
Radiographic features
Plain radiograph
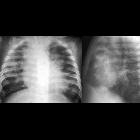
Chest radiographs will demonstrate some or all of the following features:
- cystic or linear radiolucencies in the interstitium radiating from the hilum
- affected segment is often hyperexpanded and static in volume on multiple radiographs
- pneumothorax, pneumomediastinum, or pneumopericardium
- in supine patients, pneumomediastinum is evident by the sharp mediastinum sign
- the heart tends to get smaller as intrathoracic pressure increases and results in diminished venous return into the chest
CT
- not usually part of the routine investigation (unnecessary risk of radiation exposure)
- shows cystic radiolucencies in the affected segment
- may characteristically show a line and dot pattern with pulmonary arterial branches surrounded by radiolucent air
- may help differentiate persistent PIE from a hyperlucent mass such as congenital lobar emphysema, congenital pulmonary airway malformation (CPAM)
- allows better visualization of a pneumothorax or pneumomediastinum
- if incidentally detected in adults, it may appear as perivascular lucent or low-attenuating haloes and small cysts
Treatment and prognosis
Switching from conventional to high-frequency ventilation is commonly performed in infants with pulmonary interstitial emphysema (PIE). Many cases resolve spontaneously. Frequent radiographs may be performed to assess for complications such as pneumothorax or pneumomediastinum.
Selective bronchial intubation, lobectomy and pneumonectomy are rarely used to treat progressive PIE .
Differential diagnosis
General imaging differential considerations include:
- partially treated respiratory distress syndrome (surfactant deficiency)
- partial clearing of collapsed alveoli may be seen with treatment of respiratory distress syndrome with exogenous surfactant; this pattern of alternating distended and collapsed alveoli can mimic PIE
- bronchopulmonary dysplasia
- similar bubble like lucencies; PIE typically occurs abruptly in the first week of life, BPD is more gradual and manifests later
- congenital pulmonary airway malformation (CPAM)
- typically present at birth; cysts are more variable in size and static on serial radiographs
- congenital lobar emphysema
- hyperlucent, hyperexpanded lobe; vessels may appear attenuated
- congenital diaphragmatic hernia
- larger hyperlucencies corresponding to gas in herniated bowel loops, mass effect
See also
- neonatal respiratory distress (causes)
- pulmonary infiltration with eosinophilia (sometimes also - confusingly - abbreviated as PIE)
Siehe auch:
- Pneumothorax
- Lungenemphysem
- acute respiratory distress syndrome (ARDS)
- kongenitale pulmonale Atemwegsmalformation (CPAM)
- Mediastinalemphysem
- kongenitales lobäres Emphysem
- kongenitale Zwerchfellhernie
- Pneumoperikard
- Bronchopulmonale Dysplasie
- Komplikationen bei interstitiellem Lungenemphysem
und weiter:


 Assoziationen und Differentialdiagnosen zu interstitielles Lungenemphysem:
Assoziationen und Differentialdiagnosen zu interstitielles Lungenemphysem: