intramurales Hämatom der Aorta













Aortic intramural hematoma (IMH) is an atypical form of aortic dissection due to hemorrhage into the wall from the vasa vasorum without an intimal tear. It is part of the acute aortic syndrome spectrum.
Epidemiology
Typically aortic intramural hematomas are seen in older hypertensive patients. The same condition may also develop as a result of blunt chest trauma with aortic wall injury or a penetrating atherosclerotic ulcer .
Clinical presentation
The clinical features of IMH are those of the acute aortic syndromes, namely chest pain radiating to the back and hypertension.
Pathology
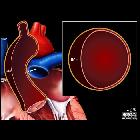
This condition is thought to begin with spontaneous rupture of the vasa vasorum, the blood vessels that penetrate the outer half of the aortic media from the adventitia and arborize within the media to supply the aortic wall .
The hematoma propagates along the medial layer of the aorta.
Consequently, intramural hematoma weakens the aorta and may progress either to outward rupture of the aortic wall or to inward disruption of the intima, the latter leading to a communicating aortic dissection .
Classification
Similar to aortic dissections, intramural hematomas are classified according to the Stanford classification :
- type A: involves the ascending aorta, with or without descending aortic involvement
- type B: confined to the descending aorta, distal to the origin of the left subclavian artery
The DeBakey classification can also be used .
Radiographic features
CT
Acute intramural hematomas appear as focal, crescentic, high-attenuating (60-70 HU) regions of eccentrically thickened aortic wall on non-contrast CT (high-attenuation crescent sign). Narrow window width is essential for identifying subtle lesions . Intimal calcification may be displaced inwards, best appreciated on the non-contrast phase.
The lesions exhibit low attenuation in relation to the aortic lumen on post-contrast CT and can be far more subtle, hence a non-contrast phase before CTA is often done in an acute aortic syndrome protocol. Unlike aortic dissection, no intimal flap is present on the CTA.
Echocardiography
An intramural hematoma (IMH) may be readily visualized with transesophageal echocardiography, which offers superior visualization of the aorta than is usually available via transthoracic examinations. Defining features include :
- crescentic thickening of the aortic wall
- normal aortic wall thickness < 3 mm
- wall thickness must exceed 7 mm to diagnose IMH
- wall demonstrates mixed echogenicity
- predominantly echodense with scattered internal echolucencies
- no internal flow detectable
- color flow Doppler interrogation important to differentiate from aortic dissection
- the true lumen of a dissection will demonstrate systolic flow
- variable flow patterns may be present in a false lumen, which tends to expand in size during diastole
- color flow Doppler interrogation important to differentiate from aortic dissection
- lack of an intimal (dissection) flap
- the luminal surface in IMH tends to be smooth and continuous
Other modalities
MRI may also detect the abnormality but conventional angiography will not.
Treatment and prognosis
If an intramural hematoma involves the ascending aorta (Stanford A), treatment is surgical to prevent rupture and progression to a classic aortic dissection.
Conservative management is indicated for an intramural hematoma of the descending aorta (Stanford B).
- 77% of intramural hematomas regress at 3 years
- survival of >90% at 5 years
Untreated, an intramural hematoma can be life-threatening as it can lead to:
Differential diagnosis
The main differential diagnoses are:
- thrombosed false lumen in classic aortic dissection: typically spirals longitudinally around the aorta whereas an intramural hematoma usually maintains a constant circumferential relationship with the aortic wall
- aortitis: typically shows concentric uniform thickening of the aortic wall with or without peri-aortic inflammatory stranding, whereas an intramural hematoma is often eccentric in configuration
Siehe auch:
- Aortendissektion
- thorakale Aortenverletzungen
- stumpfes Thoraxtrauma
- intramurales Hämatom
- Aortentrauma
- Zeichen der ummantelten Aorta
und weiter:


 Assoziationen und Differentialdiagnosen zu intramurales Hämatom der Aorta:
Assoziationen und Differentialdiagnosen zu intramurales Hämatom der Aorta:


