Internukleäre Ophthalmoplegie





Internuclear ophthalmoplegia (INO) describes a clinical syndrome of impaired adduction in one eye with dissociated horizontal nystagmus of the other abducting eye, due to a lesion in the medial longitudinal fasciculus (MLF) ipsilateral to the eye unable to adduct. It is a common finding in multiple sclerosis, but has a number of other etiologies.
Clinical presentation
Patients present with impaired adduction in one eye with dissociated horizontal nystagmus of the other abducting eye, classically with preserved convergence . However, with more extensive brainstem involvement, 'INO plus' syndromes may also be present:
- one-and-a-half syndrome: INO combined with a conjugate gaze paralysis in the other direction such that one eye fails to adduct on attempted lateral gaze (‘the half’) and may have dissociated horizontal nystagmus on abduction, while and the other eye neither adducts nor abducts (‘the one’)
- wall-eyed bilateral internuclear ophthalmoplegia (WEBINO): bilateral primary position exotropia, bilateral INO, loss of convergence, and occasionally vertical gaze deficits (e.g. vertical gaze-evoked nystagmus)
Pathology
The anatomy of the MLF and related structures in the brainstem is complex. In order to initiate horizontal eye movements, a signal is generated from the frontal eye fields (Brodmann area 8) contralateral to the direction of gaze . This is sent to its contralateral pontine CN VI nucleus via the paramedian pontine reticular formation (PPRF) . The CN VI nucleus sends motor neurons via CN VI to innervate the ipsilateral lateral rectus muscle, but also sends interneurons that cross the midline of the brainstem and form a white matter tract known as the MLF . The interneurons in MLF connect to the motor neurons of the contralateral midbrain medial rectus subnucleus of the CN III nucleus which then innervates the contralateral medial rectus muscle via CN III .
Thus, a midbrain or pontine lesion of the MLF results in the ipsilateral medial rectus subnucleus of the CN III nucleus not receiving signals from the contralateral CN VI nucleus, resulting in impaired ipsilateral adduction . The dissociated horizontal nystagmus in the non-affected abducting eye can be explained by Hering’s law of equal innervation, whereby in this case, the 'weak' medial rectus prompts the cortex to increase innervation to it . This results in additional increased, and therefore excessive, innervation to the contralateral lateral rectus causing horizontal nystagmus during abduction .
The 'INO plus' syndromes result from more extensive brainstem lesions:
- one-and-a-half syndrome: an extensive pontine lesion involving the MLF and also either the CN VI nucleus or PPRF on the side of the eye with complete conjugate gaze palsy
- wall-eyed bilateral internuclear ophthalmoplegia (WEBINO): an extensive midbrain lesion involving the bilateral MLF and nearby neurons of the medial rectus subnucleus, although there is contention regarding the accuracy of this neurophysiology
Etiology
A number of etiologies have been implicated in INO and 'INO plus' syndromes :
- brainstem demyelination (commonly bilateral): multiple sclerosis, neuromyelitis optica
- brainstem infarction (commonly unilateral): midbrain infarction, pontine infarction (e.g. facial colliculus syndrome)
- rare causes:
- brainstem tumors: midbrain or pontine tumors
- brainstem hemorrhage or hematoma
- uncal herniation
- cerebral vasculitis (e.g. secondary to systemic lupus erythematosus)
- trauma
- Arnold-Chiari malformation
- infection
- nutritional disorders: Wernicke encephalopathy, vitamin B12 deficiency
- metabolic disorders: hepatic encephalopathy, maple syrup urine disease, Fabry disease
- drugs: tricyclic antidepressants, phenothiazines, narcotics, lithium, barbiturates, propranolol
- degenerative conditions: progressive supranuclear palsy
Furthermore, a pseudointernuclear ophthalmoplegia can be seen in conditions causing complex ophthalmoplegia such as myasthenia gravis or Miller Fisher syndrome .
Radiographic features
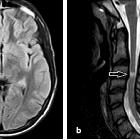
Highly variable and depend on the etiology, but the lesion will be affecting the medial midbrain or pons of the brainstem .
Treatment and prognosis
Highly variable and depend on the etiology .
Siehe auch:
- Encephalomyelitis disseminata
- Ponsblutung
- Neuromyelitis optica
- Ponsinfarkt
- kavernöses Hämangiom im Pons
- Fasciculus longitudinalis medialis
- Colliculus-facialis-Syndrom
- pontine Tumoren
- Metastasen im Pons
und weiter:


 Assoziationen und Differentialdiagnosen zu Internukleäre Ophthalmoplegie:
Assoziationen und Differentialdiagnosen zu Internukleäre Ophthalmoplegie: