hypertrophic osteoarthropathy













Hypertrophic osteoarthropathy (HPOA) is a syndrome characterized by periosteal reaction of the long bones without underlying bone lesion. There are a broad range of manifestations, although typically there is symmetrical involvement of the appendicular skeleton. Accompanying abnormal soft tissue proliferation is variable and may result in clubbing of the fingers and toes.
Hypertrophic osteoarthropathy is largely considered a secondary phenomenon, and nearly always (95-97% of cases) occurs in the setting of a wide variety of other cardiopulmonary, gastrointestinal, endocrine, hematologic, and inflammatory conditions . When associated with cancer, it is considered a paraneoplastic syndrome. A primary form, pachydermoperiostosis, is due to a heritable genetic mutation that results in similar clinical manifestations, although tend to have more soft tissue findings .
Terminology
Hypertrophic osteoarthropathy has been given various names including Pierre-Marie syndrome, Bamberger syndrome, osteoarthropatia hypertrophica, Mankowsky syndrome, and Hagner syndrome.
"Hypertrophic osteoarthropathy" may refer to either the primary or secondary syndrome, although general usage implies the secondary form, given the rarity of primary hypertrophic osteoarthropathy (also known as pachydermoperiostosis).
"Hypertrophic pulmonary osteoarthropathy" specifically refers to hypertrophic osteoarthropathy in the setting of lung disease, and not from other intrathoracic processes such as mediastinal or pleural disease .
Clinical presentation
Hypertrophic osteoarthropathy has a variable clinical presentation, ranging from asymptomatic morphologic and radiographic findings to pain accompanying the changes of the fingers and toes .
Pathology
The primary form of hypertrophic osteoarthropathy is due to mutations in the genes encoding 15-hydroxyprostaglandin dehydrogenase and solute carrier organic anion transporter family member 2A1, resulting in abnormal accumulation of prostaglandin E2 .
Although the cause of secondary hypertrophic osteoarthropathy is not established, a similar mechanism involving abnormally elevated levels of circulated hormones has been proposed as a potential etiology. Alternatively, neurogenic etiology has been proposed .
Associated disease states include:
- lung
- bronchogenic carcinoma
- non-small cell lung cancer is the strongest malignant association, particularly squamous cell cancer
- pulmonary lymphoma
- lung abscess
- bronchiectasis
- pulmonary metastases (especially from osteosarcoma)
- pleural fibroma
- mesothelioma
- cyanotic congenital heart disease
- bronchogenic carcinoma
- gastrointestinal tract and liver
- idiopathic
Radiographic features
Plain radiograph
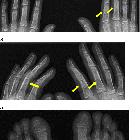
Typically seen as long bone metaphyseal and diaphyseal smooth periosteal reaction.
With disease progression, periostitis becomes more prominent or multilayered and extends to the epiphyses.
Nuclear medicine
Tc-99m MDP bone scan
symmetric linear increase in tracer accumulation along diaphyseal and metaphyseal surfaces of long bones
Treatment and prognosis
The success of treatment depends on whether the hypertrophic osteoarthropathy is due to a primary or a secondary cause.
Most success and rapid regression of hypertrophic osteoarthropathy is achieved in cases where the underlying cause is identified and treated; such as in lung tumor treated by surgical resection, radiotherapy and/or chemotherapy.
The results are less successful in the presence of metastatic disease.
In primary hypertrophic osteoarthropathy (or in cases where the underlying condition could not be treated), symptomatic relief can be obtained by use of NSAIDs, corticosteroids or bisphosphonates .
Differential diagnosis
General imaging differential considerations include:
- pachydermoperiostosis (primary hypertrophic osteoarthropathy)
- chronic venous insufficiency
- thyroid acropachy
- hypervitaminosis A
- voriconazole induced periostitis
Consider the differential for a smooth periosteal reaction.
On bone scintigraphy, differentials include:
- normal variant
- lateral cortices of the tibiae often appear with a symmetric linear uptake
- shin splints
- can appear similar, but confined to the tibiae
- chronic venous insufficiency
- can cause symmetrical periosteal uptake
- usually confined to the lower extremities below the knees
Lymphedema on its own is not known to cause hypertrophic osteoarthropathy.
Siehe auch:
- Bronchiektasen
- Lungenkarzinom
- Osteosarkom
- Lungenabszess
- solitärer fibröser Tumor der Pleura
- Mesotheliom
- Lungenmetastasen
- Chronisch-entzündliche Darmerkrankungen
- Lymphom pulmonale Manifestation
- primäre hypertrophe Osteoarthropathie
- nichtkleinzelliges Lungenkarzinom
- Zöliakie
- Hyperostose
- thyreoidale Akropachie
- Osteomyelitis sclerosans Garré
- paraneoplastisches Syndrom
- Zyanotischer Herzfehler
- Osteoperiostitis
- smooth periosteal reaction
- primär biliäre Cholangitis
- Morbus Whipple
und weiter:


 Assoziationen und Differentialdiagnosen zu hypertrophe Osteoarthropathie:
Assoziationen und Differentialdiagnosen zu hypertrophe Osteoarthropathie: