bronchiectasis






































Bronchiectasis (plural: bronchiectases) is defined as an irreversible abnormal dilatation of the bronchial tree. It has a variety of underlying causes, with a common etiology of chronic inflammation. High-resolution CT is the most accurate modality for diagnosis.
Epidemiology
As there are many causes of bronchiectasis, which may occur at essentially any age, no single demographic is particularly involved. Two groups make up the majority of cases: post-infectious and cystic fibrosis .
Clinical presentation
Bronchiectasis typically presents with recurrent chest infections, productive cough more than 8 weeks, production of copious amounts of sputum, and hemoptysis.
Pathology
Etiology
Bronchiectasis is the common response of bronchi to a combination of inflammation and obstruction/impaired clearance. Causes include :
- idiopathic (most common)
- impaired host defenses
- cystic fibrosis (CF) (most common cause in children)
- primary ciliary dyskinesia, e.g. Kartagener syndrome, Young syndrome
- primary immunodeficiency disorder, e.g. common variable immunodeficiency, hypogammaglobulinaemia, chronic granulomatous disease
- HIV/AIDS
- postinfective (most common known non-CF cause in adults)
- bacterial pneumonia and bronchitis, e.g S. aureus, H. influenzae, B. pertussis
- mycobacterial infection, e.g. tuberculosis, Mycobacterium avium-intracellulare complex
- allergic and autoimmune
- allergic bronchopulmonary aspergillosis (ABPA)
- connective tissue disease, e.g. rheumatoid arthritis , Sjögren syndrome, systemic lupus erythematosus (SLE)
- inflammatory bowel disease
- obstruction
- severe obstructive lung disease: asthma or chronic obstructive pulmonary disease (COPD)
- neoplasm, e.g. bronchial carcinoid, bronchogenic carcinoma
- inhaled foreign bodies
- congenital
- bronchial tree malformations, e.g. Mounier-Kuhn syndrome, Williams-Campbell syndrome, pulmonary sequestration, bronchial atresia
- alpha-1-antitrypsin deficiency
- others
- chronic aspiration
- traction bronchiectasis due to diffuse lung disease, e.g. pulmonary fibrosis
- radiation-induced lung disease
- post-transplantation
A mnemonic to remember common causes is CAPT Kangaroo has Mounier-Kuhn.
Subtypes
According to macroscopic morphology, three types have been described, which also represent a spectrum of severity :
- cylindrical bronchiectasis
- bronchi have a uniform caliber, do not taper and have parallel walls (tram track sign and signet ring sign)
- commonest form
- varicose bronchiectasis
- relatively uncommon
- beaded appearances where dilated bronchi have interspersed sites of relative narrowing
- cystic bronchiectasis
- severe form with cyst-like bronchi that extend to the pleural surface
- air-fluid levels are commonly present
According to one study, the relative prevalence of bronchiectatic changes were:
- cylindrical: ~ 47%
- varicose: ~ 9.9%
- cystic: ~ 45.1%
- multiple types: ~ 24.3%
Additionally, bronchiectasis can result from the traction of fibrotic lung surrounding an airway. This is known as traction bronchiectasis.
There is dilation of bronchi and bronchioles due to elastic tissue and smooth muscle destruction.
Radiographic features
Plain radiograph
Chest x-rays are usually abnormal but are inadequate in the diagnosis or quantification of bronchiectasis. Tram-track opacities are seen in cylindrical bronchiectasis, and air-fluid levels may be seen in cystic bronchiectasis. Overall there appears to be an increase in bronchovascular markings, and bronchi seen end-on may appear as ring shadows . Pulmonary vasculature appears ill-defined, thought to represent peribronchovascular fibrosis .
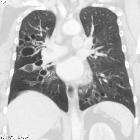
CT
CT and HRCT especially excel at demonstrating the airways and is able to a greater or lesser degree to distinguish some of the various underlying causes.
A number of features are helpful in diagnosing bronchiectasis :
- bronchus visualized within 1 cm of the pleural surface
- especially true of lung adjacent to costal pleura
- most helpful sign for early cylindrical change
- lack of tapering
- increased bronchoarterial ratio
- diameter of a bronchus should measure approximately 0.65-1.0 times that of the adjacent pulmonary artery branch
- between 1 and 1.5 may be seen in normal individuals, especially those living at high altitude
- greater than 1.5 indicates bronchiectasis
A number of ancillary findings are also recognized:
- bronchial wall thickening: normally wall of bronchus should be less than half the width of the accompanying pulmonary artery branch
- mucoid impaction
- air-trapping and mosaic perfusion
- bronchial arterial enlargement
Signs described on CT include:
Treatment and prognosis
In general, the treatment of bronchiectasis is medical and involves promoting sputum clearance, using positional physiotherapy, and early and aggressive treatment of pulmonary infections. In some cases, chronic prophylactic administration of antibiotics may be required.
In cases where bronchiectasis is severe and significant morbidity is present, surgical resection of the affected lobe may be of the benefit provided adequate respiratory reserve exists.
In cases where both lungs are extensively involved (e.g. cystic fibrosis) lung transplantation can be considered .
Differential diagnosis
The differential is in two parts:
- causes of a particular distribution of bronchiectasis
- mimics of bronchiectasis
Causes of a particular distribution of bronchiectasis
- central bronchiectasis
- upper lobe bronchiectasis
- middle lobe bronchiectasis
- lower lobe bronchiectasis
Mimics of bronchiectasis
Conditions that may mimic cystic bronchiectasis include :
- Langerhans cell histiocytosis (LCH)
- lymphangiomyomatosis (LAM)
- lymphocytic interstitial pneumonitis (LIP)
- pulmonary manifestations of AIDS
- pneumocystis pneumonia (PCP)
- emphysema
- cystic pulmonary metastases
Siehe auch:
- signet ring sign
- Lymphangioleiomyomatose
- Kartagener-Syndrom
- Pneumocystis jiroveci Pneumonie
- lymphozytisch interstitielle Pneumonie
- primäre ciliäre Dyskinesie
- angeborene Tracheobronchomegalie
- lower lobe bronchiectasis
- upper lobe bronchiectasis
- central bronchiectasis
- Emphysem
- pulmonary manifestations of AIDS
- zystische Lungenmetastasen
- middle lobe bronchiectasis
und weiter:
- mosaikartige Verdichtungen der Lunge
- Pierre-Marie-Bamberger-Krankheit
- Allergische bronchopulmonale Aspergillose
- verdickte interlobuläre Septen
- multiple zystische Lungenherde
- Alpha-1-Antitrypsin-Mangel
- zystische Fibrose
- Bronchiolitis
- Mukoidimpaktion
- tree in bud-Muster
- pulmonary Mycobacterium avium complex infection
- cystic bronchiectasis
- radiation-induced pulmonary fibrosis
- Traktionsbronchiektasen
- diffuse idiopathische pulmonale neuroendocrine Zellhyperplasie
- causes of pulmonary arterial hypertension
- pulmonale Manifestationen rheumatoide Arthritis
- Swyer-James-Syndrom
- bronchial arterial aneurysm
- congenital cystic bronchiectasis
- diffuse panbronchiolitis
- tracheobronchiale Papillomatose
- zylindrische Bronchiektasen
- Mittellappen-Syndrom
- Bronchozele
- isolated unilateral absence pulmonary artery (IUAPA)
- interstitial lung pattern
- juvenile laryngotracheal papillomatosis
- bunch of grapes
- chronische Aspirationspneumonie
- conditions with a lower lobe predominance (mnemonic)
- Nichttuberkulöse Mycobakteriose
- Nichttuberkulöse Mykobakteriose Lunge
- bronchiectasis (mnemonic)
- bronchiectasis complicated with pyopneumothorax
- Ursachen für Perfusionsdefekte in der Lungenventilations / -perfusionsszintigraphie


 Assoziationen und Differentialdiagnosen zu Bronchiektasen:
Assoziationen und Differentialdiagnosen zu Bronchiektasen: 






