pituitary microadenoma









Pituitary microadenomas are a minority of all pituitary adenomas, but can pose imaging and management challenges on account of their size and protean clinical presentations.
By definition, a microadenoma is less than 10 mm in size. If the same tumor is greater than 10 mm in size, it is then considered a pituitary macroadenoma. Differences in presentation and imaging merely represent a difference in size rather than any fundamental difference in biology.
For a general discussion, including epidemiology, treatment and prognosis, please refer to the article on pituitary adenomas.
Clinical presentation
A pituitary microadenoma is confined to the sella, and as such has no scope to produce symptoms due to mass effect. As such they are most frequently diagnosed as the result of investigating hormonal imbalance (usually excess production of one or more hormones). Rarely they can be incidental findings, however, by their very nature microadenomas are difficult to identify on anything other than dedicated pituitary imaging.
Radiographic features
Plain radiograph and CT
Historically, before the advent of MRI, the pituitary was imaged with lateral skull x-rays (looking for remodeling of the pituitary fossa), and later with CT. Although CT was able to detect up to 80-90% of microadenomas between 5-10 mm in size, it was a highly specialized technique, radiologist-dependent, and had difficulty in identifying smaller nodules .
MRI
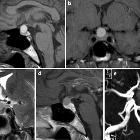
MRI is the mainstay of imaging for pituitary microadenomas and requires dedicated pituitary sequences (thin slice, small field of view, dynamic contrast acquisition). Contrast-enhanced MRIs have a sensitivity of 90%.
Post-contrast and especially thin-section dynamic contrast-enhanced imaging is an important part of a pituitary MRI and has significantly improved diagnostic accuracy . However, subtle morphology changes may still be identified on non-contrast images. These include bulkiness of the gland on the side of the microadenoma, subtle remodeling of the floor of the sella and deviation of the pituitary infundibulum away from the adenoma .
- T1: usually isointense to normal pituitary
- T1 C+ (Gd)
- dynamic sequences demonstrate a rounded region of delayed enhancement compared to the rest of the gland
- delayed images are variable, ranging from hypo-enhancement (most common) to isointense to the rest of the gland, to hyperintense (retained contrast)
- T2: variable, but often a little hyperintense
An important fact of life needs to be kept in mind when reporting pituitary MRIs: small pituitary incidentalomas are relatively common, with up to 2-30% of autopsies identifying small asymptomatic microadenomas .
Angiography (DSA)
Inferior petrosal sinus sampling
Inferior petrosal sinus sampling is now reserved for one of two situations where patients are suspected of having a pituitary microadenoma, despite normal MRI:
Differential diagnosis
The differential is broadly that of other pituitary regions masses, but is predominantly composed of:
- normal pituitary gland
- especially the periphery of the pituitary can be challenging to image
- Rathke's cleft cyst
- no enhancement rather than hypo-enhancement
- craniopharyngioma
- rarely purely intrasellar
- usually present larger
- calcification common
- pituitary metastasis
- rare
Siehe auch:
- Rathke Zyste
- Hypophyse
- Tumoren der Hypophysenregion
- Makroadenom Hypophyse
- Kraniopharyngeom
- Hypophysenadenom
- inferior petrosal sinus sampling
- purely intrasellar pituitary mass
- Inzidentalom
- prolactinoma
- Metastasen in der Hypophyse
und weiter:


 Assoziationen und Differentialdiagnosen zu Mikroadenom Hypophyse:
Assoziationen und Differentialdiagnosen zu Mikroadenom Hypophyse: