ureterocele















































 nicht verwechseln mit: periureterales Divertikel der Harnblase (Hutch-Divertikel)
nicht verwechseln mit: periureterales Divertikel der Harnblase (Hutch-Divertikel)Ureteroceles represent abnormal congenital dilatation of the distal-most portion of the ureter. The dilated portion of the ureter may herniate into the bladder secondary to the abnormal structure of vesicoureteric junction (VUJ).
Epidemiology
A ureterocele occurs in about 1 in 5000 to 1 in 12000 children and most commonly seen in the Caucasian population . Females are 4-7 times more commonly affected than males. Bilateral ureteroceles are seen in 10% of cases only .
Most ureteroceles are congenital, usually associated with the ectopic insertion of the ureter with associated duplicated collecting system (see below).
In a minority of cases, ureteroceles are an isolated abnormality, and these are usually seen in adults (see below).
Pathology
The most accepted theory is a failure in the regression of the Chwalla membrane which is a membrane between the urogenital sinus and the developing ureteral bud.
Genetics
Most cases have a sporadic occurrence.
Location and classification
Ureteroceles are classified by location. The most common system of classification is that of the urologic division of the American Academy of Pediatrics . Both types are the result of cystic ectasia of the subepithelial portion of the ureter as it enters the bladder:
- intravesical: occur at the normal vesicoureteric junction position
- extravesical: occur ectopically low and medial, near bladder neck/urethra
They pose a challenge for diagnosis and treatment because of the wide variety of anatomical abnormalities that may exist and the non-specific symptoms that patients present with.
Intravesical ureterocele (~25%)
Also known as "simple" or "orthotopic" ureterocele . Considerably less common than the ectopic variety and is almost always confined to the adult population. There is a congenital prolapse of a dilated distal ureter into the bladder lumen. Where they do occur in children, they usually cause symptoms. Bilateral in about 30% of cases .
Extravesical ureterocele (~75%)
Also known as "ectopic" ureterocele . Almost always associated with a duplicated collecting system and the result of abnormal embryogenesis. There is an abnormality in the early development of the intravesicular ureter, the ipsilateral kidney and its collecting system . It is significantly more common than the simple type.
Approximately 80% of cases are unilateral and may cause obstruction to the entire renal tract because of prolapse into the bladder neck causing bladder outlet obstruction. Additionally, ureteroceles may contain calculi.
A cecoureterocele is a subtype of extravesical ureterocele which extends inferiorly to involve the urethra. Rarely, it may herniate into the urethra and present as a perineal mass .
Radiographic features
Ultrasound
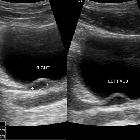
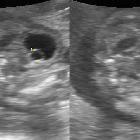
A ureterocele appears as a cystic structure projecting into the bladder, often near the normal location of the vesicoureteric junction (VUJ). This is ectopic in the majority of cases and therefore not at the expected location of the ureteric orifice. The associated ureter is usually noticeably dilated.
Fluoroscopy
IVP
Detectable findings include:
- filling defect in the bladder (cobra head sign) which may be distended, collapsed or even everted
- radiolucent halo effect
- an everted ureterocele will appear like a bladder diverticulum
MCUG
Voiding cystourethrogram may show:
- a round or oval lucency near the trigone
- there may be effacement of the defect with increasing filling of the bladder
Complications
- progression to obstructive cystic renal dysplasia
Treatment and prognosis
The prognosis of ureterocoeles is related to the degree of associated reflux or obstruction. Depending on the size and position of a ureterocele, they may prolapse into the ureter causing complete bladder obstruction.
Differential diagnosis
General imaging differential considerations include:
- pseudoureterocele
- obstruction and dilatation of an otherwise normal intramural ureter
- thick, irregular halo in the urinary bladder
- no protrusion of ureter into the bladder lumen
- bladder diverticulum
- the ureterocele is everted
Siehe auch:
- Doppelniere
- Harnblasendivertikel
- pseudoureterocoele
- periureterales Divertikel der Harnblase (Hutch-Divertikel)
- Ureterklappen
- Ureterozele bilateral
und weiter:
- vesicoureteric junction
- genitourinary curriculum
- animal and animal produce inspired signs
- multizystische Nierendysplasie
- fetal hydronephrosis
- Anhydramnion
- Obstruktive Uropathie
- Divertikel der Urethra
- Weigert-Meyer Regel
- causes of urinary bladder diverticulae
- ektope Ureterozele
- cobra head sign
- Ureterozele mit Harnleiterstein und Einblutung
- adder head sign
- spring onion sign
- prenatal hydronephrosis
- orthotope Ureterozele
- beidseitige Single-System-Ureterozelen
- vesicoureteral junction
- Single-System-Ureterozelen
- vesicoureteric junction (VUJ)
- ureterocoele: infant
- multiseptated ureterocele


 Assoziationen und Differentialdiagnosen zu Ureterozele:
Assoziationen und Differentialdiagnosen zu Ureterozele:


