papillary thyroid carcinoma





































Papillary thyroid carcinoma (PTC) is the most common malignancy of the thyroid gland and frequently has nodal metastases at presentation.
Terminology
When the tumor measures <1 cm, the term micropapillary carcinoma (mPTC) is used .
Epidemiology
Papillary thyroid cancer (as is the case with follicular thyroid cancer) typically occurs in the middle-aged, with a peak incidence in the 3 and 4 decades. It is more common in women with an M:F ratio of 1:2.5 (range 1:1.6-3:1) .
It accounts for the majority (~70%) of all thyroid neoplasms and 85% of all thyroid cancers . There are 45,000 cases in the United States every year and this type of carcinoma has the fastest increasing incidence of any malignancy in the thyroid. Those at risk include family history and previous head/neck radiation.
Clinical presentation
Presentation is usually with a solitary palpable thyroid mass.
Papillary carcinoma has a tendency to metastasize early to local lymph nodes, with 50% (39-90% ) of patients having nodal involvement at presentation (c.f. 10% for follicular thyroid cancer). These metastases are usually to the ipsilateral jugular chain (87.8%) and are usually confined to the mid and lower lymph node levels, level III and IV (73.2%) .
In ~20% of patients, lymph node metastases are the first presentation. In 50% of children and 20% of adults a cervical lymph node is palpable at the time of diagnosis .
Distal haematogenous dissemination is less common than with follicular cancer, with a prevalence of only in 5-10% of patients at presentation.
Pathology
Lymphatic spread is more common than haematogenous spread (c.f. follicular thyroid carcinoma) and multifocality is common.
Histology
Histologically papillary carcinoma demonstrates 'delicate stalks of epithelial cells' which account for its name. Cells have characteristic Orphan Annie eye nuclear inclusions, and psammoma bodies are common.
Variants
Several variants have been described according to biological behavior
- aggressive
- tall cell variant
- columnar cell variant
- hobnail variant
- less favorable
- solid variant
- diffuse sclerosing variant
- favorable
- follicular variant / encapsulated variant
- cribriform variant / morula variant
- Warthin like variant
Associations
- Gardner syndrome
- Cowden syndrome
- familial adenomatous polyposis: usually associated with the cribriform-morular variant
Radiographic features
Imaging of the neck of a patient with papillary thyroid carcinoma involves both examination of the thyroid as well as careful assessment of the regional lymph nodes for the presence of metastases.
Ultrasound
Papillary carcinoma within the thyroid usually appears as a solitary mass usually with an irregular outline, located in the subcapsular region and demonstrating vascularity . Small punctate regions of echogenicity representing microcalcifications (psammoma bodies) may be present .
Lymph node metastases have a tendency to completely cavitate (40%), and although usually multiple, in a minority of cases (6%) a single completely cystic node may be present . They tend to have septations, mural nodules and relatively thick walls .
Fine needle aspiration
Any thyroid nodule presents a diagnostic challenge as up to 50% of the general population will have thyroid nodules of some description on high-resolution thyroid ultrasound. There has previously been great variance in investigating thyroid nodules with some operators routinely aspirating thyroid lesions while others use traditional discriminators such as size in deciding whether or not to proceed to needle biopsy.
Recent research in North America, Korea, and Europe has demonstrated that traditional discriminators are poor correlates for thyroid cancer, which is most commonly papillary. Guidelines have now been produced to broadly categorize nodules as benign, indeterminate, or suspicious for malignancy with a shift in focus to looking at ultrasound appearances rather than simply size.
The U-classification system is an example proposed by the British Thyroid Association.
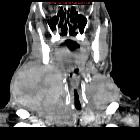
CT
CT is best at staging lymph node involvement (see thyroid cancer staging). Involved lymph nodes tend to have :
- cystic components: ~35%
- thick nodular walls: ~40%
- septae: ~60%
- purely cystic nodes are uncommon and more frequent in young patients
- calcification may be seen occasionally
- the so-called lateral aberrant thyroid is actually a lymph node metastasis from papillary thyroid carcinoma
MRI
MRI, although probably more sensitive than CT, is nonetheless still far from perfect with a sensitivity of only 67% . This is largely a result of the fact that as many as half involved nodes found histologically following surgery, being less than 3 mm in diameter .
As discussed above, nodes have a tendency to become cystic. The cystic component will have near-fluid attenuation. The solid metastatic component will appear :
General signal characteristics include:
- T1
- hypointense to muscle
- enhancement is best seen with fat suppression
- T2: variable
- hypointense: 34%
- isointense: 45%
- hyperintense: 21%
Nuclear imaging
Papillary thyroid cancer usually concentrates radioiodine, but not pertechnetate.
- FDG-PET
- FDG-avid
- incidental FDG-avid thyroid nodules have approximately 40% risk of being a primary thyroid malignancy .
Treatment and prognosis
Treatment involves both surgical resection and administration of radioactive iodine for lymph node metastases.
Overall papillary carcinoma carries a relatively good prognosis with a 20 year survival rate of approximately 90%. The 5 year survival is in the range of 95%. If the tumor is confined to the gland then mortality is less than 2.5%, with a sharp increase in mortality in patients with extension beyond the gland, to 38% .
There is a paucity of high quality data on the extent of surgery required (thyroid lobectomy versus total thyroidectomy) for low risk papillary thyroid cancer . A recent systematic review suggests that operative approach did not impact overall survival .
Differential diagnosis
Other thyroid neoplasms should be considered in the absence of cavitary cervical lymph nodes.
The differential of a cystic neck mass(es) includes:
- thyroglossal duct cyst (only if single)
- branchial cleft cyst (only if single)
- cystic metastasis to the thyroid
- abscess including tuberculous lymphadenitis
- multiple neurofibromas


 Assoziationen und Differentialdiagnosen zu papilläres Schilddrüsenkarzinom:
Assoziationen und Differentialdiagnosen zu papilläres Schilddrüsenkarzinom: 





