coarctation of the aorta





































Coarctation of the aorta (CoA) refers to a narrowing of the aortic lumen.
Epidemiology
Coarctations account for between 5-8% of all congenital heart defects. They are more frequent in males, M:F ratio of ~2-3:1.
Clinical presentation
Varies accordingly to the degree of stenosis and the associated abnormalities. Patients may be asymptomatic in a setting of non-severe stenosis.
Children and adults can present with angina pectoris and leg claudication. On clinical examination, diminished femoral pulses and differential blood pressure between upper and lower extremities may be noted.
ECG
- high left ventricular voltage (HLVV)
- voltage criteria present for left ventricular hypertrophy
- left ventricular "strain" pattern
- variably present in the lateral leads (I, aVL, V5-6)
- asymmetric T-wave inversion originating from a depressed ST segment
- right ventricular hypertrophy
- less common
Pathology
It can be primarily divided into two types:
- characterized by diffuse hypoplasia or narrowing of the aorta from just distal to the brachiocephalic artery to the level of ductus arteriosus
- typically with a more discrete area of constriction just proximal to the ductus but distal to the origin of the left subclavian artery
- therefore, the blood supply to the descending aorta is via the patent ductus arteriosus
- characterized by a short segment abrupt stenosis of the post-ductal aorta
- it is due to thickening of the aortic media and typically occurs just distal to the ligamentum arteriosum (a remnant of the ductus arteriosus)
Associations
As with many congenital abnormalities, coarctation of the aorta is associated with other congenital anomalies.
- cardiac
- bicuspid aortic valve: most common associated defect and seen in 75-80%
- ventricular septal defect
- cyanotic congenital lesions including
- truncus arteriosus
- transposition of the great arteries, especially with a sub-pulmonic VSD and overriding pulmonary artery (Taussig-Bing)
- mitral valve defects including
- hypoplastic mitral valve
- parachute mitral valve
- abnormal papillary muscles
- patent ductus arteriosus
- non cardiac
- intracranial berry aneurysms
- spinal scoliosis
- syndromic associations
- cardiac
- wider syndromic
- PHACE syndrome
- Turner syndrome: a coarctation can be seen in 15-20% of those with Turner syndrome
Radiographic features
Plain radiograph
- figure of 3 sign: contour abnormality of the aorta
- inferior rib notching: Roesler sign
- secondary to dilated intercostal collateral vessels which form as a way to bypass the coarctation and supply the descending aorta
- the dilated and tortuous vessels erode the inferior margins of the ribs, resulting in notching
- seen only in long standing cases, and therefore not seen in infancy (unusual in patients <5 years of age)
- seen in 70% of cases presenting in older children or adults
- if the coarctation is distal to either subclavian artery, then increased flow occurs through the subclavian artery, forming a collateral pathway via the internal thoracic artery, anterior intercostal artery, posterior intercostal artery and then into the descending thoracic aorta
- usually the 4 to 8 ribs are involved; occasionally involves the 3rd to 9th ribs
- as the 1st and 2nd posterior intercostal arteries arise from the costocervical trunk (a branch of the subclavian artery) and do not communicate with the aorta, these are not involved in collateral formation, and the 1st and 2nd ribs do not become notched
- if bilateral rib notching: the coarctation must be distal to the origin of both subclavian arteries, to enable bilateral collaterals to form
- if unilateral right rib notching
- then the coarctation lies distal to the brachiocephalic trunk but proximal to the origin of the left subclavian artery
- or there may be a right sided aortic arch with aberrant left subclavian artery distal to coarctation
- collaterals cannot form on the left, as the left subclavian is distal to the coarctation
- if unilateral left rib notching, then this suggests an associated aberrant right subclavian artery arising after the coarctation
- the coarctation is distal to the origin of the left subclavian artery, therefore collaterals form on the left
- collaterals cannot form on the right, as the aberrant right subclavian artery arises after the coarctation
Antenatal ultrasound
Useful in assessing for infantile coarctations. The suprasternal notch-long axis views are considered helpful. The fetal right ventricle can be appear enlarged in severe coarctations although this alone is not a specific feature. Occasionally an aortic arch view may directly show a narrowing.
Echocardiography
Best visualized from the suprasternal window with transthoracic echocardiography and the upper esophageal positions with a transesophageal approach. Features commonly present include :
- reduction in luminal caliber of the descending aorta
- often accompanied by post-stenotic dilatation
- demonstrates sudden increase in velocity as measured by pulsed wave Doppler
- the continuous wave Doppler envelope will demonstrate the characteristic "shark tooth" morphology
- sharply elevated systolic peak
- diastolic velocity profile markedly concave
- the continuous wave Doppler envelope will demonstrate the characteristic "shark tooth" morphology
- left ventricular hypertrophy
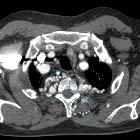
Angiography: CTA/MRA/DSA
All modalities are capable of delineating the coarctation as well as collateral vessels, most common collateral pathway being subclavian artery to internal mammary artery to intercostal arteries (resulting in inferior rib notching) to post-coarctation part of descending thoracic aorta.
Treatment and prognosis
The urgency of treatment depends on the presence of congestive cardiac failure. This is usually the case in severe coarctations found in infancy. In less severe cases, elective treatment when the child is older (typically ~2 years of age) is preferred .
Treatment can be either primary surgical repair with excision of the coarctation and end-to-end anastomosis, or balloon angioplasty. Subclavian flap repair is a common surgical technique used, where the origin and proximal left subclavian artery is excised, opened up and sutured onto the aorta. If the subclavian is ligated, it is usually anastomosed onto the left common carotid artery.
Complications
- neonatal heart failure
- subarachnoid hemorrhage from a ruptured berry aneurysm
- aortic dissection
- infective endocarditis: in the context of an added infective insult
- mycotic aneurysm: in the context of an added infective insult
Differential diagnosis
Imaging differential considerations include:
- pseudo-coarctation of the aorta: elongation, narrowing or kinking with no pressure gradient or collateral formation, no rib notching
- chronic large vessel arteritis, e.g. chronic phase of Takayasu arteritis
Siehe auch:
- Rippenusuren
- Takayasu-Arteriitis
- aortic pseudocoarctation
- Aortenisthmusstenose im Röntgenbild
- Mid-Aortic-Syndrom
- post-surgical pseudoaneurysm in aortic coarctation
- präduktale Aortenisthmusstenose
- Atresie der Aorta
- thorakale Aortenstenose
und weiter:
- prästenotische Dilatation
- Anomalien des Aortenbogens
- Ektasie Aorta ascendens
- Aortenisthmusstenose
- Neurofibromatose Typ 1
- Herzfehler
- Meckel-Syndrom
- Kardiomegalie
- Turner-Syndrom
- acyanotic congenital heart disease
- PHACE syndrome
- Varianten der Herzanatomie
- Bland-White-Garland-Syndrom
- hypoplastic left heart syndrome
- CXR approach to congenital heart disease
- double outlet right ventricle (DORV)
- Bikuspidalität der Aortenklappe
- 3-Zeichen bei Aortenisthmusstenose
- shone syndrome
- systemic hypertension
- Akrorenales Syndrom
- fetal right ventricular enlargement
- parachute mitral valve
- Ventrikelseptumdefekt
- chest x-ray appeoach to congenital heart disease
- congenital aortic stenosis
- dysencephalia spanchnocystica
- congenital heart disease - chest x-ray approach
- anomalous left coronary artery off the pulmonary artery
- Alagille-Syndrom
- collaborative publications by radiopaedians
- reverse figure 3 sign
- Usuren
- isolated unilateral absence pulmonary artery (IUAPA)
- Aortenisthmus
- Nicht-zyanotische Herzfehler
- Aortenaneurysma bei Kindern und Jugendlichen
- persistent fifth aortic arch
- coarctation of the aorta in children
- Aortendissektion bei Aortenisthmusstenose


 Assoziationen und Differentialdiagnosen zu Aortenisthmusstenose:
Assoziationen und Differentialdiagnosen zu Aortenisthmusstenose:


