intracardiac thrombus




















Intracardiac thrombi are seen in a variety of clinical settings and can result in severe morbidity or even death from embolic events. They can occur following myocardial infarction with ventricular thrombus formation, or with atrial fibrillation and mitral stenosis where atrial thrombi predominate.
Thrombi in the chambers of the left heart are a common source of complications like stroke and other arterial embolic syndromes.
Radiographic features
Echocardiography
Transthoracic echocardiography is the diagnostic tool of first choice. However, the inability to visualize all cardiac chambers and the reduced image quality in some patients are limitations of transthoracic echocardiography. Therefore, transesophageal echocardiography has emerged as the most sensitive modality for the detection of intracardiac thrombi .
Recently formed thrombi demonstrate homogenous echogenicity, irregular margins, and tend to be independently mobile, whereas chronic thrombi tend to be immobile. Intracardiac thrombi can be subdivided broadly as follows :
- thrombi in transit
- usually represents the embolic propagation of deep vein thrombosis
- intracavitary and freely mobile, visualized in the right atrium, right ventricle, or main pulmonary artery
- typically associated with signs of right heart strain
- may result in paradoxical embolism if an intracardiac shunt is present
- thrombi in-situ
- usually due to regional low flow states or the presence of instrumentation, such as a prosthetic valve
- left atrial thrombi
- primarily located in the left atrial appendage (LAA)
- features supportive of thrombosis of the LAA include:
- spontaneous echocontrast (SEC)
- pulsed wave Doppler measured emptying velocities less than 20 cm/s
- the presence of aliasing within the LAA with color flow Doppler and normal flow velocities argue against a low flow state, and make thrombosis unlikely
- left ventricular thrombi
- majority form adjacent to myocardium with a regional wall motion abnormality
- may form next to normokinetic myocardium in Loeffler endocarditis
- the use of contrast agents greatly improves visualization
- transthoracic windows are typically superior for the visualization of apical thrombi
- left atrial thrombi
- usually due to regional low flow states or the presence of instrumentation, such as a prosthetic valve
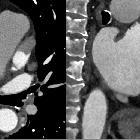
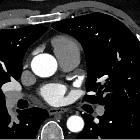
CT
The lack of enhancement differentiates cardiac thrombus from other cardiac tumors.
MRI
SSFP
Cine images using steady-state free precession (SSFP) allow the localization of the thrombus and targets following sequences to the region of interest. Cine images can also demonstrate segmental hypokinesia in surrounding infarcted myocardium. On cine images, thrombus can sometimes be difficult to separate from the adjacent myocardium if they have similar intensity and can be readily missed unless gadolinium is administered.
First pass perfusion
In this sequence, the heart is imaged at every heartbeat following pump injection of gadolinium. This allows dynamic imaging of contrast as it passes from the right ventricle, into the left ventricle, into the myocardium, and following the redistribution. Thrombus being an avascular lesion will be of homogenous low intensity on every phase.
Early gadolinium enhancement (<4 minutes)
A long inversion time of ~440 ms is chosen to null any non-vascular lesions (e.g. thrombus) that do not contain gadolinium. This accentuates thrombus by making it very hypointense compared to surrounding tissues which contain gadolinium. Any lesion which is not homogenously hypointense points to an alternative pathology.
Late gadolinium enhancement (>8 minutes)
A short inversion time is initially chosen to null the gadolinium-rich myocardium so that any areas of myocardial enhancement are accentuated. The initial inversion time is decided upon by performing a scout at different TI, and choosing the TI which nulls the myocardium. This also incidentally results in some fat suppression as fat has a short T1 value (~150 ms). The inversion time is progressively increased as late gadolinium imaging progresses, because gadolinium washes out of the myocardium, and the T1 value increases back to baseline. Thrombus will remain of low intensity, and any underlying infarct will be revealed by subendocardial enhancement.
Treatment and prognosis
The biggest risk from cardiac thrombus is distal embolization, resulting in stroke, visceral infarction or distal limb ischemia. Treatment is anticoagulation.
Differential diagnosis
When considering the diagnosis of an intracardiac thrombus, the differential for a mass in the cardiac chambers includes:
- anatomic variants
- cardiac tumors
- vegetations
- non-infectious
- infectious
Siehe auch:
- Herzspitzenaneurysma
- Herzohr Okkluder
- Herzohr Clip
- Thrombus im linken Herzohr
- Vorhofmyxom
- Tumoren des Herzens
- Myxom des linken Vorhofs
- Kontrastmittelfluss-Artefakte
- Vorhofthrombus
- Thrombus im linken Vorhof
und weiter:


 Assoziationen und Differentialdiagnosen zu intrakardiale Thromben:
Assoziationen und Differentialdiagnosen zu intrakardiale Thromben: 



