intrakranielle Lipome


















Intracranial lipomas are not tumors as such, but rather a result of abnormal differentiation of embryologic meninx primitiva. They are frequently associated with abnormal development of adjacent structures.
Epidemiology
Intracranial lipomas are congenital lesions and as such are found at any age when the brain is imaged for other reasons.
Clinical presentation
They are usually asymptomatic, and either found incidentally or as a result of investigation of related malformations and their presentation (e.g. epilepsy, hydrocephalus) .
Pathology
A number of theories have been put forward to explain the development of intracranial lipomas. The favored theory is persistence and maldifferenitation of the meninx primitiva (subarachnoid space precursor), which accounts for the subarachnoid location, associated parenchymal anomalies, and traversing structures of intracranial lipomas .
Location
Intracranial lipomas are widely distributed in the intracranial compartment. Although they can be found essentially anywhere, certain regions are characteristic:
- pericallosal lipoma (45%)
- associated with agenesis of the corpus callosum is ~50% of cases
- divided morphologically into tubonodular and curvilinear types
- quadrigeminal cistern lipoma (25%)
- associated with underdevelopment of the inferior colliculus
- suprasellar cistern lipoma (15%)
- cerebellopontine angle lipoma (10%)
- the facial nerve and vestibulocochlear nerve often courses through the lipoma
- Sylvian fissure (5%)
- choroid plexus lipoma (rare)
Radiographic features
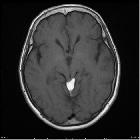
The characteristic finding on both CT and MRI is a mass which has appearances consistent with fat.
CT
On CT, they typically appear as a non-enhancing mass with uniform fat density (hence negative CT attenuation values). It has a lobulated 'soft' appearance, conforming to adjacent anatomy. Some peripheral calcification may be present.
MRI
MRI with and without fat saturation are able to make the diagnosis easily. In the absence of fat-saturated images, then chemical shift artefact may be useful. Signal characteristics are, not surprisingly, that of fat:
- T1: high signal intensity
- T2: high signal intensity
- T1 C+ (Gd): no enhancement
- fat saturated sequences: low signal
- SWI: can produce blooming due to susceptibility artifact
Often the lipomas are traversed by cranial nerves and adjacent vessels, best seen on high-resolution sequences.
Treatment and prognosis
Intracranial lipomas are in most cases asymptomatic, and even when associated with symptomatic malformations (e.g. callosal dysgenesis) they usually require no treatment per se. In fact, attempts at resection have had relatively high morbidity with little benefit . Treatment of seizures or hydrocephalus is, of course, necessary if these are present .
Differential diagnosis
The differential is essentially that of masses which contain fat, and therefore includes:
- intracranial dermoid: if ruptured will often have multiple droplets scattered through the subarachnoid space; usually midline
- intracranial teratoma
- lipomatous transformation of neoplasm: PNET, ependymoma, glioma
On MRI, if no fat saturated sequences are available then a number of other possibilities should be entertained, which also have high T1 signal.
- thrombosed berry aneurysm: often will have a calcified rim and hemosiderin staining on gradient echo or SWI sequences
- white epidermoid: rare, and will restrict on DWI
See also
Siehe auch:
- Falxlipom
- Balkenlipom
- tektales Lipom
- Ependymom
- intrakranielles Fett
- intrakraniale Teratome
- zerebellopontines Lipom (Lipom im Kleinhirnbrueckenwinkel)
- meninx primitiva
- white epidermoid
- intrakranielle Dermoidzyste
- sakkuläre zerebrale Aneurysmata
- suprasellar lipoma
- lipomatöses Meningeom
- Fett intracerebral
- Primitiver neuroektodermaler Tumor
- Pai-Syndrom (Lippenspalte - faziale Polypen - ZNS-Lipome)
- Lipome in den intrakranialen venösen Sinus
und weiter:
- Tumoren der Hypophysenregion
- suprasellar cistern lipoma
- classification system for midline abnormalities of the brain and skull
- Weichteillipom
- Spasmus hemifacialis
- intra vestibular lipoma
- intrakranielle Lipome der hinteren Schädelgrube
- pericallosal lipoma and callosal dysgenesis
- Fibrolipom des Nasenseptums
- lipoma interfering with vermian development
- Fett in den intrakranialen venösen Sinus
- Lipom am Tentorium


 Assoziationen und Differentialdiagnosen zu intrakranielle Lipome:
Assoziationen und Differentialdiagnosen zu intrakranielle Lipome:






