Klippel-Feil syndrome
















 nicht verwechseln mit: Klippel-Trénaunay-Weber-Syndrom
nicht verwechseln mit: Klippel-Trénaunay-Weber-SyndromKlippel-Feil syndrome is a complex heterogeneous entity that results in cervical vertebral fusion. Two or more non-segmented cervical vertebrae are usually sufficient for diagnosis.
Epidemiology
There is a recognised female predilection . Klippel-Feil syndrome has an incidence of 1:40,000-42,000 .
Clinical presentation
The classic clinical triad of a short neck, low hairline, and restricted neck motion is considered to be present in <50% of patients with this syndrome.
Pathology
It is believed to result from faulty segmentation along the embryo’s developing axis during the 3 to 8weeks of gestation.
Associations
- Sprengel deformity of the shoulder (see image)
- Wildervanck syndrome
- Duane syndrome
- anomalies of the aortic arch and branching vessels, e.g. carotid, subclavian arteries
- spinal scoliosis
- intervertebral disc herniation
- cervical spondylosis
- renal abnormalities, e.g. unilateral renal agenesis
Classification
There are two classifications:
1. Original classification (described by Maurice Klippel and Andre Feil): three types grouped depending on the extent and location of vertebral fusion as well as associated vertebral abnormalities :
- type I: fusion of many cervical and upper thoracic vertebrae
- type II: fusion of two or three vertebrae with associated hemivertebrae, occipito-atlantal fusion or other cervical spine abnormalities
- type III: cervical fusion with lower thoracic or lumbar vertebral fusion
2. Updated classification (by Clarke et al ) grouped by patterns of inheritance, associated anomalies, and the axial level of the most anterior fusion.
Radiographic features
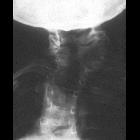
Plain radiograph
- vertebral fusion: fused facets and spinous processes
- anteroposterior narrowing of the vertebral bodies (wasp-waist sign)
- hemivertebrae
- omovertebral bone
- spina bifida
- associated scoliosis and Sprengel deformity
On flexion/extension radiographs, there will be less movement between fused segments, and increased movement between non-fused portions.
CT
CT is able to better image many of the features seen on plain radiography and in addition may demonstrate canal stenosis. Central canal narrowing is generally associated with secondary degenerative changes. It is a valuable tool to assess bony anatomy and is very helpful in pre-operative planning.
MRI
MRI is indicated in patients with neurologic deficits. It is excellent in demonstrating canal stenosis and cord compression. Disk bulge and herniation can be identified that may encroach upon and damage the spinal cord. MR imaging can also reveal associated conditions such as myelomalacia, syringohydromyelia, diastematomyelia, diplomyelia, and Chiari I malformation . Associated cord abnormalities are seen in 12% of cases .
Treatment and prognosis
No definitive treatment exists. Lifestyle modifications and preventive activities include avoidance of contact sports such as rugby. Neck braces and traction may provide symptomatic relief. Adverse sequelae such as pain despite conservative management and progressive instability may benefit from surgical decompression, with or without fusion.
History and etymology
Klippel-Feil syndrome was originally described by Maurice Klippel and Andre Feil in 1912 with patients having a triad of:
Differential diagnosis
Differentials for the fused appearances of the cervical spine include:
- ankylosing spondylitis
- complications of discitis: chronic
- surgical fusion: absence of wasp-waist sign and fusion of facet joints and spinous processes are helpful clues
- juvenile idiopathic arthritis
Siehe auch:
- Blockwirbel
- Skoliose
- Blockwirbel Halswirbelsäule
- Sprengel-Deformität
- Os omo-vertebrale
- Srb-Anomalie
- wasp-waist sign
- Wildervanck syndrome
- Nielsen-Syndrom
- Karotisagenesie
und weiter:
- Rippenanomalien
- Basiläre Impression
- Syrinx
- angeborene Wirbelanomalien
- Syringomyelie
- kongenitale Radiusköpfchenluxation
- Synostose
- Mondini-Dysplasie
- congenital ossicular anomalies
- iniencephaly
- Grisel-Syndrom
- Spondylodese Atlas - Axis
- atlantookzipitale Fusion
- cervico-ocular-acoustic dysplasia
- kongenitale Anomalien der Halswirbelsäule


 Assoziationen und Differentialdiagnosen zu Klippel-Feil-Syndrom:
Assoziationen und Differentialdiagnosen zu Klippel-Feil-Syndrom:





