Syrinx













Syrinx (pl. syringes) is the collective name given to hydromyelia, syringomyelia, syringobulbia, syringopontia, syringomesencephaly, and syringocephalus.
Terminology
The use of the general term 'syrinx' has grown out of the difficulty in distinguishing between hydromyelia and syringomyelia using current imaging modalities.
Strictly speaking, in hydromyelia, there is dilatation of the central canal of the spinal cord, and thus the lesion is lined by ependyma. While in syringomyelia there is cystic dissection through the ependymal lining of the central canal and a CSF collection within the cord parenchyma itself, and thus this lesion is not lined by ependyma.
As clinically, there is no difference between the two and severity of symptoms is related to the location and size of the lesion the word 'syrinx' may be used as a general descriptor and has the benefit of brevity.
It is, however, worth knowing the related terms and their distinguishing features.
- hydromyelia: fluid accumulation/dilatation within the central canal, therefore, lined by ependyma
- syringomyelia: cavitary lesion within cord parenchyma, of any cause (there are many); located adjacent to the central canal, therefore not lined by ependyma
- syringohydromyelia: a term used for either of the above, since the two may overlap and cannot be discriminated on imaging, also known as hydrosyringomyelia
- syringobulbia: extension of syringomyelia into the medulla oblongata, although used by some authors to refer to any syrinx in the brainstem
- syringopontia: extension of syringomyelia into the pons
- syringomesencephaly: extension of syringomyelia into the midbrain
- syringocephalus: extension of syringomyelia into the cerebrum, also known as syringoencephalomyelia
- syrinx: common name for the cavity in all of the above
Clinical presentation
Neurological symptoms vary considerably depending on where the syrinx is located in the neuraxis. Classically there is a mix of motor and sensory features, with both acute and chronic effects.
See the individual articles on syringomyelia, syringobulbia, syringopontia, syringomesencephaly, and syringocephalus for further details of the clinical presentation.
Pathology
As mentioned, a syrinx refers to any cavity within the spinal cord which may or may not communicate with the central canal. When a syrinx is present rostrally into the neuraxis, syringomyelia is generally also present and the resultant syrinx is generally appreciated as an 'extension' from this.
Etiology
They may be congenital (90%) or acquired in etiology.
Congenital causes include:
- myelomeningocele
- Chiari I malformation
- Chiari II malformation
- Dandy-Walker malformation
- Klippel-Feil syndrome
Acquired (secondary) causes include:
- post-traumatic: occurs in ~5% of patients with spinal cord injury usually from a whiplash-type injury; symptoms may start many months or years after an injury
- cervical canal stenosis
- post-inflammatory
- secondary to a spinal cord tumor
- secondary to a hemorrhage
- due to vascular insufficiency
Radiographic features
Radiographic investigations may reveal many anomalies depending on the cause of the syrinx. This section will solely describe the imaging characteristics of the syrinx itself.
Plain radiograph
Plain films of the spine may show a subtle widening of the spinal canal in both the sagittal and coronal planes.
CT
The syrinx may be appreciated as an area of decreased attenuation, similar to that of CSF, within the spinal cord.
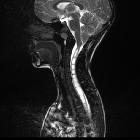
MRI
The syrinx follows CSF signal characteristics on all sequences:
- T1: hypointense
- T2: hyperintense, although there may be hypointense regions representing flow or pulsation artifact
It is worth noting that unless the cause of the syrinx is obvious, then imaging with contrast on the first study is prudent to ensure a small enhancing tumor is not present.
Treatment and prognosis
When symptomatic, neurosurgical intervention may be required.
Siehe auch:
- Chiari-Malformation Typ 1
- Klippel-Feil-Syndrom
- Arnold-Chiari-Malformation Typ 2
- Ventriculus terminalis
- Syringomyelie
- Dandy-Walker-Syndrom
- Myelomeningozele
- Hydromyelie
- Syringobulbie
und weiter:


 Assoziationen und Differentialdiagnosen zu Syrinx:
Assoziationen und Differentialdiagnosen zu Syrinx:






