Dandy Walker malformation















Dandy-Walker malformation (DWM) is the most common posterior fossa malformation, characterized by the triad of:
- hypoplasia of the vermis and cephalad rotation of the vermian remnant
- cystic dilatation of the fourth ventricle extending posteriorly
- enlarged posterior fossa with torcular-lambdoid inversion (the torcula lying above the level of the lambdoid due to abnormally high tentorium)
Terminology
This article focuses on the "classic" presentation of Dandy-Walker malformation, please refer to Dandy-Walker continuum for a discussion on other related posterior fossa malformations.
The term “classic Dandy-Walker malformation” and others like “Dandy-Walker variant” or “Dandy-Walker complex”, were created to differentiate those malformations that do not meet the criteria for Dandy-Walker malformation, however, some authors recommend to avoid them as they have a lack of specificity that may create some confusion. Instead, a more detailed anatomic description is recommended .
Epidemiology
The estimated prevalence of a Dandy-Walker malformation and related variants is about 1 per 30,000 live births and accounts for ~7.5% (range 4-12%) of the cases of infantile hydrocephalus. It is known as the most common posterior fossa malformation .
Clinical presentation
Clinical presentation is dependent on the severity of the abnormality. In a classic Dandy-Walker malformation, patients usually manifest in the first year of life with symptoms of hydrocephalus and associated neurological symptoms. Macrocephaly is the most common manifestation and in ~80% of cases, the diagnosis is made by the first year of life. Despite severe cerebellar abnormalities, cerebellar signs are not common.
Pathology
Many have a sporadic inheritance with some possibly having an autosomal dominant or X-linked inheritance.
Associations
- non-syndromic CNS: in ~70% of cases other CNS abnormalities are present, including
- cortical dysplasia, polymicrogyria, or subependymal grey matter heterotopia
- dysgenesis of the corpus callosum
- lipoma of the corpus callosum
- holoprosencephaly
- schizencephaly
- occipital encephalocele: less than 5%
- lumbosacral meningocele
- syringomyelia
- non-syndromic non-CNS: found in ~25% of patients
- cleft palate
- facial angiomas
- low-set ears
- polydactyly or syndactyly
- cardiac anomalies
- syndromic non-aneuploidic associations
- aneuploidic associations
- Emanuel Syndrome
- trisomy 18
- trisomy 13
- triploidy
Radiographic features
Ultrasound
Antenatal sonographic features that would suggest the diagnosis include the combination of :
- marked enlargement of the cisterna magna (≥10 mm)
- complete aplasia of the vermis
- a trapezoid-shaped gap between the cerebellar hemispheres
Antenatal ultrasound may falsely overdiagnose the condition if performed before 18 weeks, as the vermis has not properly formed.
MRI
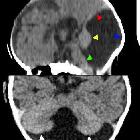
MRI is the modality of choice for assessment of Dandy-Walker malformation, although both CT and ultrasound will demonstrate the pertinent features.
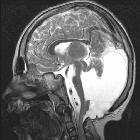
Classically Dandy-Walker malformation consists of the triad of:
- hypoplasia of the vermis and cephalad rotation of the vermian remnant
- cystic dilatation of the fourth ventricle extending posteriorly; usually the cerebellar hemispheres are displaced anterolaterally, but with a normal size and morphology
- enlarged posterior fossa with torcular-lambdoid inversion (torcular lying above the level of the lambdoid due to abnormally high tentorium)
In 75-90% of patients, obstructive hydrocephalus is evident by three months of age , in many cases due to aqueduct stenosis . CSF flow study is recommended to better assess the hydrodynamic changes and identify eventual aqueductal stenosis association, which cannot be treated by cystoperitoneal shunt placement .
Treatment and prognosis
A Dandy-Walker malformation carries a high mortality rate, ~70% in live-born fetuses, often due to associated abnormalities . It is thought to carry a poorer prognosis if diagnosed prior to 21 weeks of gestation and a better prognosis if diagnosed postnatally . A cystoperitoneal shunt could be considered in situations where hydrocephalus is significant problem. Even in the absence of any associated syndromes, there is a recurrence risk of ~2.5% (range 1-5%) in subsequent pregnancies.
History and etymology
It was initially described by Blackman and Dandy in 1914 .
Differential diagnosis
The differential is that of other causes of an enlarged CSF retrocerebellar space (and mimics thereof) including:
- mega cisterna magna
- epidermoid cyst
- arachnoid cyst
- Blake pouch cyst
- Joubert anomaly (vermian hypoplasia)
- isolated fourth ventricle
On antenatal ultrasound, also consider technical and timing factors such as:
- too steep insonation angle
- a scan performed too early in gestation, i.e. prior to 18 weeks
Siehe auch:
- Mega Cisterna magna
- Arachnoidalzysten der hinteren Schädelgrube
- Blake's-Pouch-Zyste
- Dandy-Walker variant
- Joubert-Syndrom
- Dandy Walker continuum
- classification system for malformations of the cerebellum
- vermis hypoplasia
- pädiatrische Erkrankungen des Liquorsystems
und weiter:
- Arachnoidalzyste
- Syrinx
- Dandy-Walker continuum
- Isolated inferior vermian hypoplasia
- lemon sign
- Meckel-Syndrom
- Syringomyelie
- Meningoenzephalozele
- Coffin-Siris syndrome
- intraspinale zystische Läsionen
- Entwicklungsstörungen des Ventrikelsystems
- Kleinhirnhypoplasie
- dysencephalia spanchnocystica
- Salonen-Herva-Norio syndrome
- zerebelläre Anomalien
- hydrolethalus
- Ritscher-Schinzel-Syndrom
- zystische Malformationen der hinteren Schädelgrube
- Backenzahn-Zeichen (ZNS)
- kongenitaler Hydrozephalus


 Assoziationen und Differentialdiagnosen zu Dandy-Walker-Syndrom:
Assoziationen und Differentialdiagnosen zu Dandy-Walker-Syndrom: