Neoplasien der Cauda equina

MRI Imaging
features of spinal myxopapillary ependymoma. Sagittal T2W (precontrast) image showing solid lobulated hyperintense intradural lesion with tiny haemorrhagic foci in its superior pole.
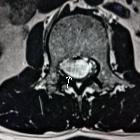
MRI Imaging
features of spinal myxopapillary ependymoma. Axial T2W (precontrast) image at L2 level.

MRI Imaging
features of spinal myxopapillary ependymoma. Sagittal T1W image (precontrast) showing hypointense lesion.

MRI Imaging
features of spinal myxopapillary ependymoma. Sagittal T1W (postcontrast) image showing avid homogenous intralesional contrast enhancement.

MRI Imaging
features of spinal myxopapillary ependymoma. Axial T1W (Post contrast) image.

MRI Imaging
features of spinal myxopapillary ependymoma. Sagittal T2W (precontrast) image of entire spine showing no any similar lesions within cervical and dorsal spine.

Spinal
ependymoma in a patient with Kabuki syndrome: a case report. Spine MRI, sagittal pre-operative and post-operative images. Sagittal pre-operative TSE T2 WI (a) and T1 WI with Gd (b) show a lumbar endocanalar mass extending from L3 to L4, isointense on T1 and T2 WI with peripheral contrast enhancement. Sagittal post-operative TSE T2 WI (c) and T1 WI with Gd (d) show total resection of the tumor

MRI Imaging
features of spinal myxopapillary ependymoma. Sagittal STIR (precontrast) image showing lesion morphology and extent.

Spinal
schwannoma • Schwannoma (intrathecal) - Ganzer Fall bei Radiopaedia

Teratoma •
Cystic teratoma of the conus - Ganzer Fall bei Radiopaedia

Spinal
neuroendocrine tumor • Cauda equina neuroendocrine tumor - Ganzer Fall bei Radiopaedia

Lymphoma of
the spinal cord • Intradural lymphoma - Ganzer Fall bei Radiopaedia

Neoplasms of
the cauda equina (differential) • Spinal leptomeningeal metastases - Ganzer Fall bei Radiopaedia

Capillary
hemangioma of cauda equina: a case report. Post-gadolinium enhancement revealed in sagital (A), coronal (B), and axial (C) magnetic resonance images of this lesion.

Myxopapillary
ependymoma • Myxopapillary ependymoma - Ganzer Fall bei Radiopaedia


Coexistence
of intervertebral disc herniation with intradural schwannoma in a lumbar segment: a case report. Gadolinium contrast MR images (a coronal image, b sagittal image) demonstrated a partially enhanced intradural mass at the left side of the L3/4 spinal canal. Axial image (c) showed an intradural mass of heterogeneous signal at the left and a herniated disc at the right extradural space

Coexistence
of intervertebral disc herniation with intradural schwannoma in a lumbar segment: a case report. T2-weighted sagittal image (a) revealed L3/4 disc herniation which compressed the dural sac from the right side. Two slices away, there was a hyperintense intradural mass at the same level (b). T1-weighted sagittal image (c) demonstrated a hypointense mass behind the L3/4 intervertebral disc

Capillary
hemangioma of cauda equina: a case report. Sagital magnetic resonance images showing an intradural mass at the level of L3, isointense to spinal cord on T1-weighted (A) and iso-hyperintense on T2-weighted sequences (B). T1-weihted axial image demonstrating the intradural mass pushing the caudal roots to the side of the canal (C).

Capillary
hemangioma of cauda equina: a case report. Plain radiography of lumbar area showing bony erosion and widening of the canal (scalloping) at the level of L3 vertebra (arrow).

Spinal
dermoid cyst • Cystic teratoma of the conus - Ganzer Fall bei Radiopaedia
The differential diagnosis for masses of the cauda equina region is often considered separately to the remainder of the spinal cord. It is often difficult to determine whether masses in this region are intramedullary or intradural-extramedullary.
Most common tumors
- myxopapillary ependymoma
- by far the most common tumor of the conus medullaris and filum terminale, representing more than 90% of tumors in this region
- most commonly present in young adult males
- marked homogeneous enhancement is typical
- often have associated hemorrhage; may calcify or undergo cystic degeneration
- if large, may expand the spinal canal, cause scalloping of the vertebral bodies and extend out of the neural exit foramina
- schwannoma
- second most common tumor in this region
- most are solitary and sporadic, however, there is an association with neurofibromatosis type 2
- small tumors may be distinguished from myxopapillary ependymomas by their origin from nerve roots (myxopapillary ependymomas arise from the filum terminale)
- virtually all enhance
- hemorrhage may occur but less commonly than with myxopapillary ependymoma
- may be associated with intrinsic vascular changes (thrombosis; sinusoidal dilatation), cyst formation and fatty degeneration
Less common tumors
- paraganglioma
- although spinal paragangliomas occur almost exclusively in the cauda equina, they represent only 3.5-3.8% of neoplasms in this region
- serpentine flow voids are typically seen along the surface of and within the tumor nodule (however, flow voids may also be seen in hemangioblastomas)
- hemorrhage is common, leading to a "cap sign" on T2 weighted images
- the characteristic “salt-and-pepper” appearance of neck and skull base paragangliomas may be seen
- intense enhancement is virtually always present
- intradural metastases
- lesions are often multiple
- “sugar coating” of the spinal cord and nerve roots may be seen
- in the pediatric population, they are most commonly “drop metastases” from a CNS primary; in adults, non-CNS primary tumors are more common
- hemangioblastoma
- focal flow voids, especially in larger lesions
- vivid enhancement
- an associated tumor cyst or syrinx is common (50-100%)
- mostly sporadic however there is an increased incidence in patients with von Hippel-Lindau syndrome (multiple lesions are typical)
- meningioma
- occurrence within the conus/cauda equina is uncommon
- usually isointense with the spinal cord on T1 and T2 weighted images
- calcification may be present (calcified lesions are hypointense on T1 and T2 weighted images, may show only minimal enhancement)
- hemorrhage is uncommon
- there is an increased incidence in patients with neurofibromatosis type 2
- astrocytoma
- isolated conus medullaris involvement is seen in 3%. Involvement of the filum terminale is rare
- the vast majority enhance
- hemorrhage is uncommon
- spinal PNET
- the most common sites of spinal involvement are the filum terminale and cauda equina (57%)
- diffuse heterogeneous enhancement pattern
- because CSF seeding commonly occurs, leptomeningeal enhancement may be seen
- ganglioglioma
- only rarely involve the conus medullaris
- predominantly in children and young adults
- mixed signal intensity on T1 weighted images (due to the dual cellular elements of the tumor)
- most demonstrate patchy enhancement
- calcification is common
Benign masses that mimic tumors
- lipoma of the filum terminale
- common (present in up to 5% of the general population )
- usually an incidental finding, however, may be associated with signs and symptoms of tethered spinal cord
- signal follows that of fat on all sequences (hyperintense on T1 and T2, saturation on fat saturated sequences)
- no enhancement
- can demonstrate chemical shift artefact on T2* / gradient weighted sequences
- dermoid cyst
- 20% are located in the cauda equina
- patients are usually younger than 20 years of age
- usually contain fatty elements
- no enhancement or mild rim enhancement
- epidermoid cyst
- similar intensity to CSF on T1 and T2 weighted images
- typically non-enhancing, however, a thin rim of contrast enhancement may be seen
- diffusion restriction on DWI
Siehe auch:
- Gangliogliom
- Schwannom
- Paragangliom
- Hämangioblastom
- Astrozytom
- epidermale Inklusionszyste
- Cauda equina Lipom
- spinale Epidermoidzyste
- spinales Ependymom
- Cauda-equina-Syndrom
- spinales Ependymom des Filum terminale
- Schwannom der Cauda equina
- epidermoid cyst of the cauda equina
- intraspinale Tumoren
- spinal primitive neuroectodermal tumours
- Paragangliom an der Cauda equina
- Hämangiom der Cauda equina
- sugar coating
- intradural metastases
und weiter:


 Assoziationen und Differentialdiagnosen zu Neoplasien der Cauda equina:
Assoziationen und Differentialdiagnosen zu Neoplasien der Cauda equina:








