pulmonary edema












Pulmonary edema is a broad descriptive term and is usually defined as an abnormal accumulation of fluid in the extravascular compartments of the lung .
Clinical presentation
The clinical presentation of pulmonary edema includes:
- acute breathlessness
- orthopnea
- paroxysmal nocturnal dyspnea (PND)
- foaming at the mouth
- distress
Pathology
One method of classifying pulmonary edema is as four main categories on the basis of pathophysiology which include:
- increased hydrostatic pressure edema
- two pathophysiological and radiological phases are recognized in the development of pressure edema
- these phases are virtually identical for left heart failure and fluid overload
- permeability edema with diffuse alveolar damage (DAD)
- permeability edema without diffuse alveolar damage (DAD)
- mixed edema due to simultaneous increased hydrostatic pressure and permeability changes
Etiology
Broadly causes can be classified as cardiogenic and non-cardiogenic:
- cardiogenic pulmonary edema:
- left heart failure
- mitral regurgitation
- aortic stenosis
- arrhythmias
- myocardial pathology
- non-cardiogenic pulmonary edema:
- fluid overload
- pulmonary edema with acute asthma
- postobstructive pulmonary edema / postintubation pulmonary edema/negative pressure pulmonary edema
- pulmonary edema in pulmonary thromboembolism
- pulmonary edema due to air embolism
- pulmonary veno-occlusive disease
- near-drowning pulmonary edema / asphyxiation pulmonary edema
- ARDS: pulmonary edema with diffuse alveolar damage
- heroin-induced pulmonary edema
- pulmonary edema following administration of cytokines
- transfusion-related acute lung injury
- high-altitude pulmonary edema
- neurogenic pulmonary edema
- reperfusion pulmonary edema
- pulmonary edema following lung transplantation
- re-expansion pulmonary edema
- post-pneumonectomy pulmonary edema
- post lung volume reduction pulmonary edema
- pulmonary edema from anti-snake venom administration
- activity-related
- swimming-induced pulmonary edema
- immersion pulmonary edema
- exercise-induced pulmonary edema
- acute selenium toxicity
The causes of non-cardiogenic pulmonary edema can be recalled with the following mnemonic: NOTCARDIAC.
Radiographic features
Plain radiograph
The chest radiograph remains the most practical and useful method of radiologically assessing and quantifying pulmonary edema .
Features useful for broadly assessing pulmonary edema on a plain chest radiograph include:
- upper lobe pulmonary venous diversion (stag's antler sign)
- increased cardiothoracic ratio/cardiac silhouette size: useful for assessing for an underlying cardiogenic cause or association
- features of pulmonary interstitial edema:
- peribronchial cuffing and perihilar haze
- septal (Kerley) lines
- thickening of interlobar fissures
- features of pulmonary alveolar edema:
- air space opacification classically in a batwing distribution
- may have air bronchograms
- pleural effusions and fluid in interlobar fissures (including 'vanishing' pulmonary pseudotumor)
There is a general progression of signs on a plain radiograph that occurs as the pulmonary capillary wedge pressure (PCWP) increases (see pulmonary edema grading). Whether all or only some of these features can be appreciated on the plain chest radiograph, depend on the specific etiology . Furthermore, pulmonary edema is usually a bilateral process, but it may uncommonly appear to be unilateral in certain situations and pathologies (see unilateral pulmonary edema).
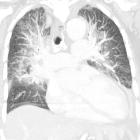
CT
Interstitial pulmonary edema is most commonly demonstrated by the following CT signs :
- ground glass opacification
- bronchovascular bundle thickening (due to increased vascular diameter and/or peribronchovascular thickening)
- interlobular septal thickening
Alveolar edema is demonstrated by airspace consolidation in addition to the above findings.
Pleural effusions are a frequent accompanying finding in cardiogenic/hydrostatic pulmonary edema.
Ultrasound
The appearance of pulmonary edema is defined as a function of the perturbation of the air-fluid level in the lung, a spectrum of appearances coined the alveolar-interstitial syndromes.
As subpleural interlobular septa thicken among air-filled alveoli, they create a medium in which incident ultrasound waves will reverberate within, creating a short path reverberation artifact. Referred to as B-lines, these are pathological when more than three appear, garnering the title lung rockets, and consistent with thickened interlobular septa. When spaced 7 mm apart they correlate with radiographic interstitial edema and when 3 mm apart with ground glass opacification. When surrounding alveoli become fluid-filled, the resultant interface assumes a tissue-like pattern. The tissue-like sign and shred sign are pathognomonic .
Differential diagnosis
General imaging differential considerations include other causes of diffuse airspace opacification:
- diffuse pulmonary hemorrhage: has no dependent gradient and usually no pleural effusion
- diffuse pneumonia : usually no dependent gradient
- pulmonary alveolar proteinosis: usually no pleural effusion
See also
Siehe auch:
- pulmonalvenöse Stauung
- Schmetterlingsödem
- diffuse Lungenblutung
- einseitiges Lungenödem
- pulmonary oedema grading
und weiter:
- Bronchopneumogramm
- Lymphangiosis carcinomatosa
- Konsolidierung der Lunge
- Kerley-Linien
- right middle lobe consolidation
- acute respiratory distress syndrome (ARDS)
- upper lobe pulmonary venous diversion
- verdickte interlobuläre Septen
- Alveolarproteinose
- peri-bronchial cuffing
- subpleurale Retikulationen
- Goodpasture-Syndrom
- rheumatic heart disease
- crazy paving-Muster
- komplette Verschattung Hemithorax
- retikuläres Muster
- adult chest radiograph common exam pathology
- TRALI
- Surfactant-Mangelsyndrom
- subpleural line
- acute bilateral airspace opacification
- acute hypersensitivity pneumonitis
- Reexpansionslungenödem
- Lungenödem nach Lungenvolumenreduktion
- Kerley lines in the exam
- interstitielles Lungenödem
- höhergradige Stauungszeichen
- nicht-kardiogenes Lungenödem
- Lungenödem nach Lungentransplantation
- Schmetterlingskonfiguration von Lungenverdichtungen
- Lungenödem nach Pneumektomie
- unilateral pulmonary edema after rapid re-expansion of spontaneous pneumothorax
- focal pulmonary opacity (mnemonic)
- Höhenlungenödem
- laryngospasm-induced pulmonary oedema
- Einschwemmsyndrom (TUR-Syndrom)
- Pulmonalvenenthrombose
- neurogenes Lungenödem
- post lung transplantation pulmonary oedema
- iatrogene Überwässerung
- Niederdruck-Lungenödem
- Herzinsuffizienz
- akutes Herzversagen
- salt water aspiration
- heroin induced pulmonary oedema
- kardiogenes Lungenödem
- reimplantation response
- pulmonales perivaskuläres Ödem
- near drowning pulmonary oedema
- Lungenödem neonatal
- reperfusion pulmonary oedema
- pulmonary oedema due to air embolism
- pulmonary oedema with acute asthma


 Assoziationen und Differentialdiagnosen zu Lungenödem:
Assoziationen und Differentialdiagnosen zu Lungenödem:

