Rheumatoid arthritis (musculoskeletal manifestations)

































Rheumatoid arthritis (RA) is a chronic multi-system disease with predominant musculoskeletal manifestations. Being a disease that primarily attacks synovial tissues, RA affects synovial joints, tendons, and bursae.
Refer to the related articles for a general discussion of rheumatoid arthritis and for the particular discussion of its respiratory manifestations.
Radiographic features
Regarding disease detection, as the early RA manifestations are non-osseous in nature, ultrasound and MRI have shown to be superior to radiographs and CT. Plain radiography, however, remains the mainstay of imaging in the diagnosis and follow-up of RA .
Plain radiograph
One large cohort study showed that radiographically demonstrable erosions were present in 30% of patients at diagnosis, and in 70% three years later .
The radiographic hallmarks of rheumatoid arthritis are:
- erosions; important early finding, in the “bare areas”, frequently in the radial side of the metacarpophalangeal (MCP) joints
- soft tissue swelling
- fusiform and periarticular; it represents a combination of joint effusion, edema and tenosynovitis
- this can be an early/only radiographic finding
- osteoporosis: initially juxta-articular, and later generalized; compounded by corticosteroid therapy and disuse
- joint space narrowing: symmetrical or concentric
Hands and wrists
Diagnosis and follow-up of patients with RA commonly involve imaging of the hands and wrists. The disease tends to affect the proximal joints in a bilaterally symmetrical distribution.
RA is a synovial based process, with a predilection for:
- PIP and MCP joints (especially 2 and 3 MCP)
- ulnar styloid
- triquetrum
As a rule, the DIP joints are spared.
Late changes include:
- subchondral cyst formation: the destruction of cartilage presses synovial fluid into the bone
- subluxation causing:
- ulnar deviation of the MCP joints
- boutonniere and swan neck deformities
- hitchhiker’s thumb deformity
- carpal instability: scapholunate dissociation, ulnar translocation
- ankylosis
- scallop sign: erosion of the ulnar aspect of the distal radius which may be predictive of extensor tendon rupture (Vaughan-Jackson syndrome)
Elbow
- joint effusion (elevated fat pads)
- joint space narrowing
- periarticular erosions
- cystic changes
Feet
- similar to the hands, there is a predilection for the PIP and MTP joints (especially 4and 5 MTP)
- involvement of subtalar joint
- posterior calcaneal tubercle erosion
- hammertoe deformity
- hallux valgus
Shoulder
- erosion of the distal clavicle
- marginal erosions of the humeral head: the superolateral aspect is a typical location
- reduction in the acromiohumeral distance: "high-riding shoulder" due to subacromial-subdeltoid bursitis and high incidence of rotator cuff tear
Hip
- concentric loss of joint space, compared with osteoarthritis (OA) where there is a tendency for superior loss of joint space
- acetabular protrusio
Knee
- joint effusion
- typically involves the lateral or non-weight bearing portion of the joint
- loss of joint space involving all three compartments
- lack of subchondral sclerosis and osteophytes, compared with OA
- prepatellar bursitis
Spine
The cervical spine is frequently involved in RA (in approximately 50% of patients), whereas thoracic and lumbar involvement is rare. Findings include:
- erosion of the dens
- atlantoaxial subluxation
- atlantoaxial distance is more than 3 mm on a flexion radiograph
- atlantoaxial impaction (cranial settling): cephalad migration of C2
- erosion and fusion of uncovertebral (apophyseal joints ) and facet joints
- osteoporosis and osteoporotic fractures
- erosion of spinous processes
Ultrasound
Sonography can assess the soft tissue manifestations of RA. In particular:
- synovial proliferation and inflammation of the superficial joints
- tenosynovitis: extensor carpi ulnaris tendon involvement is common in early disease and may lead to erosion of the ulnar styloid
- bursitis
Ultrasound also has a role in guiding corticosteroid injections in this setting.
CT
CT is not routinely used in the evaluation of peripheral RA. It has applications in imaging of the spine, and peri-operative assessment .
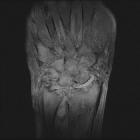
MRI
MRI is particularly sensitive to the early and subtle features of RA.
Commonly used sequences include T1-weighted contrast-enhanced spin-echo with fat saturation and T2-weighted spin-echo or gradient-echo sequences .
Features of RA best demonstrated with MRI include :
- synovial hyperemia: an indication of acute inflammation
- synovial hyperplasia (rice bodies)
- pannus formation
- decreased thickness of cartilage
- subchondral cysts and erosions:
- MRI is much more sensitive than radiography
- it is thought that subchondral cysts in RA eventually progress to erosions (i.e. constitute "pre-erosions")
- contrast enhancement may distinguish erosions or pre-erosions from degenerative subchondral cysts
- juxta-articular bone marrow edema
- joint effusions
Differential diagnosis
The differential for the skeletal manifestations of RA includes:
- degenerative osteoarthritis
- involves the: DIPs, PIPs, 1CMC joints
- non-uniform joint space loss, subchondral sclerosis, and osteophytes
- soft tissue swelling: Heberden node (DIPs) and Bouchard node (PIPs)
- no erosions and no ankylosis
- erosive osteoarthritis
- clinically acute inflammatory attacks (swelling, erythema, pain) in postmenopausal women
- typically involves the DIPs, PIPs, 1CMC joint , but not MCP joints or large joints
- classic central erosions, possible ankylosis
- psoriatic arthritis (PsA)
- commonly involves the hands and there is an interphalangeal predominant distribution in PsA compared to MCP joint predominance in rheumatoid arthritis (RA)
- starts with erosions in the margins and eventually involves the
whole joint, the classic changes being the pencil-in-cup deformity and bone proliferation (unlike RA) - osteoporosis not a feature in PsA
- MRI dynamic enhancement pattern may differentiate PsA from RA at 15 minutes
- reactive arthritis (Reiter syndrome)
- a predilection for the lower limb
- osteopenia and then osteoporosis, uniform joint space loss, subchondral cyst formation, subluxations, marginal erosions but no bone formation
- symmetrical involvement of the: PIPs, MCPs, and carpal bones
- systemic lupus erythematosus (SLE)/Jaccoud arthropathy
- joint space loss, subchondral sclerosis, osteophyte, and ulnar deviation of the phalanges without erosions
- calcium pyrophosphate dihydrate (CPPD) arthropathy
- usually only affects the MCPs: symmetric joint space narrowing, subchondral cysts, and osteophytes
- unlike RA: chondrocalcinosis and no erosions
- gout
- usually in older men
- punched out erosions usually with a sclerotic border and overhanging edges, tophi most commonly involves the 1 MTP (which is known as podagra)
Site-specific differential diagnosis:

