Rathke's cleft cyst























Rathke cleft cysts, also known as pars intermedia cysts, are non-neoplastic, sellar or suprasellar epithelium-lined cysts arising from the embryologic remnants of Rathke pouch in the pituitary gland. They are common lesions and usually incidentally identified.
Epidemiology
- common, found in ~15% (range 11-22%) of autopsies
- rare in childhood; mostly seen in adults
- since the underlying substrate is congenital, lesions thought to enlarge throughout life
- recognized female preponderance (~2:1 female to male ratio)
Clinical presentation
The vast majority of Rathke cleft cysts are asymptomatic and incidentally found.
If large, they may cause:
- visual disturbances: due to compression of the optic chiasm
- pituitary dysfunction
- due to compression of adjacent pituitary tissue and distortion of the pituitary stalk
- present in up to 69% of symptomatic cases
- headaches
Pathology
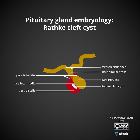
Rathke pouch forms during the 4 week of embryologic development as a rostral outpouching from the roof of the primitive oral cavity. The anterior wall of the pouch gives rise to the anterior lobe of the pituitary (pars distalis). The posterior wall of the pouch does not proliferate and remains as the intermediate lobe of the pituitary (pars intermedia). The lumen of the pouch narrows to form a cleft (Rathke cleft) that normally regresses. Persistence of this cleft with the expansion is believed to be the origin of a Rathke cleft cyst.
The wall of the cyst is typically lined by a single columnar cell layer of epithelium, often containing goblet cells, and is often ciliated. An intraluminal nodule which macroscopically appears white and is often adherent to the cyst wall (although it may be free-floating) is composed of solid tissue that represents desquamated cellular debris .
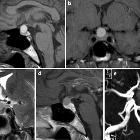
Radiographic features
On imaging, a Rathke cleft cyst is seen as a well defined non-enhancing midline cyst within the sella arising between the anterior and intermediate lobes of the pituitary. 40% are purely intrasellar and 60% have suprasellar extension. Purely suprasellar location, although reported, is rare.
Plain radiograph
On lateral skull x-ray, it can rarely cause sellar enlargement if reaches large size .
CT
- non-contrast
- typically non-calcified and of homogenous low attenuation
- uncommonly it may be of mixed iso- and low-attenuation, or contain small curvilinear calcifications in the wall (seen in 10-15% of cases)
- postcontrast
- typically non-enhancing, although the cyst wall may enhance in some cases
MRI
The signal characteristics vary according to the cyst composition, which may be mucoid or serous.
- T1
- 50% are hyperintense (high protein content)
- 50% are hypointense
- T2
- 70% are hyperintense
- 30% are iso or hypointense
- T1 C+ (Gd)
- no contrast enhancement of the cyst is seen; however, a thin enhancing rim of surrounding compressed pituitary tissue may be apparent
In ~75% of cases, a small non-enhancing intracystic nodule can be identified which is virtually pathognomonic of a Rathke cleft cyst. When seen, it is hyperintense to surrounding fluid on T1 and hypointense on T2. Depending on the signal of the surrounding fluid, it may be inapparent on one sequence or the other.
Occasionally, a fluid-fluid level may be seen (particularly if there has been a hemorrhage).
Treatment and prognosis
Surgical treatment is indicated for symptomatic cases.
A case series showed 18% recurrence rate after surgical resection, supporting the theory that a relationship exists between symptomatic Rathke cleft cyst and craniopharyngioma .
Differential diagnosis
The main differential diagnoses are:
- cystic pituitary adenoma
- can show fluid-fluid level or hemorrhagic debris; Rathke cleft cysts almost never bleed
- craniopharyngioma
- no gender difference
- similar age group
- usually suprasellar or have a suprasellar component
- tend to calcify
- arachnoid cyst
- older patients
- no gender difference
- epidermoid cyst
- usually suprasellar
- restriction on DWI
- teratoma
- usually has solid components
- often fatty signal
Siehe auch:
- Arachnoidalzyste
- Tumoren der Hypophysenregion
- Teratom
- Kraniopharyngeom
- epidermale Inklusionszyste
- Rathke's pouch
- zystische Läsionen in der Hypophyse
- Pars intermedia-Zyste der Hypophyse
- zystische Läsionen der Sellaregion
- kongenitale Anomalien der Hypophyse
- Rathke Zyste Größenzunahme
- Xanthogranulom in der Sella
- spontane Regression einer Rathke Zyste
und weiter:
- Hypophyse
- Empty-Sella-Syndrom
- Pituitary MRI (an approach)
- Mikroadenom Hypophyse
- neuroradiologisches Curriculum
- pituitary region mass with intrinsic high T1 signal
- hypothalamic lesions
- Apoplex der Hypophyse
- purely intrasellar pituitary mass
- mostly / purely cystic pituitary region masses
- cyst with dot sign
- supraselläre Arachnoidalzyste
- T2 hypointense Rathke cleft cyst


 Assoziationen und Differentialdiagnosen zu Rathke Zyste:
Assoziationen und Differentialdiagnosen zu Rathke Zyste:







