vestibular schwannoma






















































Vestibular schwannomas, also known as acoustic neuromas, are relatively common tumors that arise from the vestibulocochlear nerve (CN VIII) and represent ~80% of cerebellopontine angle (CPA) masses. Bilateral vestibular schwannomas are strongly suggestive of neurofibromatosis type 2 (NF2).
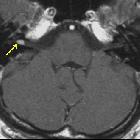
On imaging, they classically present as a solid nodular mass with an intracanalicular component that often results in widening of the porus acusticus. They usually show intense contrast enhancement and, when larger, cystic degeneration can be present. Hemorrhagic areas may also be seen, but calcification is typically not present.
Terminology
Vestibular schwannomas are commonly known as acoustic neuromas, which is a misnomer. The term vestibular schwannoma is preferred as these tumors most frequently arise from the vestibular portion of the vestibulocochlear nerve and arise from Schwann cells . A mixture of the terms, acoustic schwannoma, may also be seen.
Epidemiology
Vestibular schwannomas account for ~7.5% of all primary intracranial tumors and 75-90% of cerebellopontine angle masses . The vast majority (95%) of solitary lesions are sporadic. Bilateral vestibular schwannomas are highly suggestive of neurofibromatosis type 2 (NF2), although bilateral tumors are encountered in the familial form of vestibular schwannomas in the absence of other stigmata of NF2 .
Although they usually occur between the fourth to sixth decades of life, with a median age of 50 years , individuals with NF2 tend to be present them earlier, with a peak incidence around the third decade of life. Although rare, vestibular schwannomas may occur in children.
Clinical presentation
The typical presentation is with adult-onset sensorineural hearing loss or non-pulsatile tinnitus. In some patients, this goes unnoticed, and presentation is delayed until the lesion is much larger and presents with symptoms related to mass effect. Possibilities include cerebellar and brainstem symptoms (e.g. cranial nerve dysfunction, other than vestibulocochlear), or hydrocephalus due to effacement of the fourth ventricle.
Pathology
Vestibular schwannomas are benign tumors (WHO grade 1), which usually arise from the intracanalicular segment of the vestibular portion of the vestibulocochlear nerve (CN VIII) , near the transition point between glial and Schwann cells (Obersteiner-Redlich zone) . In over 90% of cases, these tumors arise from the inferior division of the vestibular nerve . Less than 5% cases arise from the cochlear component of the vestibulocochlear nerve (CN VIII) .
They are well-circumscribed encapsulated masses which, unlike neuromas, arise from but are separate from nerve fibers , which they usually splay and displace rather than engulf.
They can display two types of growth pattern:
- Antoni A
- elongated cells with cytoplasmic processes arranged in fascicles
- little stromal matrix
- Verocay bodies: nuclear-free zones of processes lying between regions of nuclear palisading
- Antoni B
- loose meshwork of cells
- less densely cellular
- microcysts and myxoid change
Immunohistochemical staining is usually positive for S-100 protein .
Radiographic features
Location
- most have an intracanalicular component, often widening the porus acusticus (trumpeted IAM sign) (up to 90%)
- a small "CSF cap" typically remains, separating intracanalicular tumor from the cochlea; however, growth laterally through the cochlea (transmodiolar) or vestibule (transmacular) into the middle ear may occasionally occur
- involvement of the IAC fundus is associated with decreased rates of hearing preservation
- extracanalicular extension may result in an "ice cream cone" appearance, presumed to represent tumor growth inwards along a path of least resistance
- a minority are purely extracanalicular, merely abutting the porus acusticus (~20%)
- rarely, small tumors may be confined to the labyrinth (see intralabyrinthine schwannoma)
- the location and extension can be classified according to the Koos grading scale
Tumor consistency
- small tumors tend to be solid, but larger tumors commonly demonstrate cystic degeneration
- may have hemorrhagic areas
- typically without calcification
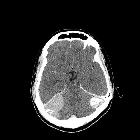
CT
May show erosion and widening of the internal acoustic canal (IAC). The density of these tumors on non-contrast imaging is variable, and often they are hard to see, especially on account of beam hardening and streak artifact from the adjacent petrous temporal bone.
Contrast enhancement is present but can be underwhelming, especially in larger lesions with cystic components. Many cysts are loculations of CSF adjacent to a vestibular schwannoma, others represent cystic degeneration within schwannomas.
MRI
- T1
- slightly hypointense to the adjacent brain (63%) or isointense to it (37%)
- may contain hypointense cystic areas
- T2
- heterogeneously hyperintense to adjacent brain
- fluid intensity cystic areas
- may have associated peritumoural arachnoid cysts
- T1 C+ (Gd)
- contrast enhancement is intense
- however, heterogeneous in larger tumors
Post-operational MRI
Linear enhancement may not indicate a tumor, but if there is nodular enhancement, suspect tumor recurrence (requires follow-up MRI).
Treatment and prognosis
There is variability in the rate of growth of vestibular schwannomas, and as such, the decision to treat requires consideration of the patient's age and co-morbidities. The options include :
- observation and follow-up
- stereotactic radiosurgery
- microsurgery: number of approaches are possible, including :
- retrosigmoid (transmeatal) (suboccipital)
- able to preserve hearing
- can be used for large tumors
- limited view of the internal auditory canal
- has a greater chance of residual tumor (in the lateral aspect of internal auditory canal)
- middle cranial fossa
- best for small intracanalicular tumors
- able to preserve hearing
- translabyrinthine
- careful skeletonisation of the facial nerve required (i.e. intraoperative facial nerve monitoring by needle electromyography with continuous stimulation)
- loss of hearing guaranteed
- retrosigmoid (transmeatal) (suboccipital)
Overall tumor recurrence is low, ranging between 1-9% .
History and etymology
The tumor was first described in 1777 by Dutch anatomist Eduard Sandifort (1742-1814) .
Schwann cells, and hence schwannomas, are named after the German physician and physiologist Theodor Schwann (1810–1882) .
The first case in which a patient survived surgical resection of a vestibular schwannoma was in 1894. The procedure was performed by British surgeon Sir Charles Balance .
Differential diagnosis
The most frequent differentials to be considered are:
- meningioma
- usually more homogeneous in appearance: significant signal heterogeneity with cystic or hemorrhagic areas is more typical of vestibular schwannomas than meningiomas (although cystic meningiomas do occur)
- meningiomas tend to have a broad dural base
- usually lack the trumpeted internal acoustic meatus sign
- large meningiomas often located asymmetrically relative to the IAC
- calcification more common
- epidermoid
- no enhancing component
- very high signal on DWI
- does not widen the internal auditory canal
- metastasis
- uncommon
- usually does not remodel the internal auditory canal, as metastases are usually present for only a short time
- ependymoma
- centered on the fourth ventricle
- does not extend into the internal auditory canal
- usually younger patients
Practical points
What the surgeon wants to know
In addition to general remarks about the size and location of the tumor, significant findings that influence surgical management include :
- how close to the fundus of the IAC the tumor reaches
- anatomical variations
- high-riding jugular bulb
- dehiscent jugular bulb
- aberrant internal carotid artery
- aberrant course of the facial nerve
- pneumatization of the petrous apex
- size and location of the sigmoid sinus
See also
Siehe auch:
- Meningeom
- Ependymom
- Schwannom
- Tumor Kleinhirnbrückenwinkel
- trigeminal schwannoma
- cystic meningioma
- cerebellopontine angle
- Epidermoid
- Meningeom des Kleinhirnbrückenwinkels
- bilaterales Vestibularisschwannom
- zystisches Schwannom des Kleinhirnbrückenwinkels
- Schwannom des Nervus facialis
- recurrent acoustic schwannoma
- trumpet IAM sign
und weiter:
- Nervus facialis
- intrakranielle Epidermoidzyste
- spinale Schwannome
- neurinoma of the trigeminal nerve
- Dural-Tail-Zeichen
- Neurofibromatose Typ 2
- intraventricular epidermoid
- Hirntumoren
- zerebellopontines Lipom (Lipom im Kleinhirnbrueckenwinkel)
- Arteria cerebelli anterior inferior
- obersteiner-Redlich zone
- trumpeted internal acoustic meatus sign
- ice-cream cone sign
- intra vestibular lipoma
- intralabyrinthine schwannoma
- facial nerve choristoma
- Bogengangtumor
- erweiterter innerer Gehörgang
- Dumbbell schwannoma
- intracanalicular acoustic schwannoma
- Schwannome der Hirnnerven
- intrakraniale Schwannome
- acoustic neurinoma presenting as subarachnoid hemorrhage


 Assoziationen und Differentialdiagnosen zu Vestibularisschwannom:
Assoziationen und Differentialdiagnosen zu Vestibularisschwannom:






