ARDS





































Respiratory distress syndrome (RDS) is a relatively common condition resulting from insufficient production of surfactant that occurs in preterm neonates.
On imaging, the condition generally presents as bilateral and relatively symmetric diffuse ground glass lungs with low volumes and a bell-shaped thorax.
Terminology
RDS is also known as hyaline membrane disease (not favored as reflects non-specific histological findings), neonatal respiratory distress syndrome, lung disease of prematurity (both non-specific terms), or as some authors prefer surfactant-deficiency disorder .
Epidemiology
The incidence is estimated at 6 per 1000 births . Uncommon after 36 weeks' gestation due to development of pneumocyte surfactant production around 35 weeks .
Clinical presentation
Respiratory distress presents in the first few hours of life in a premature baby. Signs include tachypnea, expiratory grunting, and nasal flaring. The infant may or may not be cyanosed. Substernal and intercostal retractions may be evident.
Risk factors include maternal diabetes, greater prematurity, perinatal asphyxia and multiple gestations.
Associated abnormalities are those that can occur in prematurity: germinal matrix hemorrhage, necrotizing enterocolitis, patent ductus arteriosus, delayed developmental milestones, hypothermia and hypoglycemia.
Pathology
Immature type II pneumocytes cannot produce surfactant. The lack of surfactant increases the surface tension in alveoli causing collapse. Patients have a decreased lecithin to sphingomyelin ratio. Damaged cells, necrotic cells, and mucus line the alveoli.
Although most cases are related to prematurity alone, rarely patients may have genetic disorders of surfactant production and can present in a similar clinical and radiological manner .
As the alveoli are collapsed (microscopically), the lungs are collapsed macroscopically as well. It is a diffuse type of adhesive atelectasis.
Radiographic features
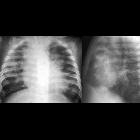
Plain radiograph
- low lung volumes are mandatory (atelectasis - lung collapse).
- diffuse granular opacities (ground glass), bilateral and symmetrical - "white lungs".
- air bronchograms may be evident.
- bell-shaped thorax.
- hyperinflation (in a non-ventilated patient) excludes the diagnosis; if the patient is intubated there might be hyperinflation.
RDS can be safely excluded if the neonate has a normal chest radiograph at six hours after birth.
If treated with surfactant therapy, there may be an asymmetric improvement.
On transabdominal ultrasound, retrodiaphragmatic hyperechogenicity can be seen. If this hyperechogenicity does not resolve by day 9-18 on follow up ultrasound, it helps in the prediction of risk of development of bronchopulmonary dysplasia .
Treatment and prognosis
Exogenous surfactant administration. Supportive oxygen therapy.
Complications
Acute
- persistent patent ductus arteriosus (PDA) due to reduced oxygen stimulus
- pulmonary interstitial emphysema (from treatment)
- oxygen toxicity (from treatment)
- pulmonary hemorrhage (can also be included in the differential diagnosis)
- air leak (barotrauma related to ventilation)
Chronic
- bronchopulmonary dysplasia
- recurrent pulmonary infection
- subglottic stenosis (from intubation)
Differential diagnosis
Consider:
- congenital heart disease
- group B Streptococcal pneumonia
- pulmonary hemorrhage
- pulmonary edema / pulmonary venous congestion
- neonatal pneumonia
- transient tachypnea of the newborn: lung volumes are normal to slightly hyperinflated in TTN and decreased in RDS
Siehe auch:
- Bronchopneumogramm
- Lungenödem
- Pankreatitis
- Persistierender Ductus arteriosus
- Herzfehler
- Lungenblutung
- fetal conditions associated with maternal diabetes
- interstitielles Lungenemphysem
- TRALI
- Bronchopulmonale Dysplasie
und weiter:
- right middle lobe consolidation
- Lungenfibrose
- Milchglasverschattungen
- crazy paving-Muster
- komplette Verschattung Hemithorax
- Parenchymband
- neonatal chest radiograph in the exam setting
- medikamenteninduzierte Pneumonitis
- acute bilateral airspace opacification
- Akute interstitielle Pneumonie
- Schock (Medizin)
- pulmonale Kryptokokkose
- PIE
- nicht-kardiogenes Lungenödem
- pulmonary manifestations of antiphospholipid syndrome
- Acute Respiratory Distress Syndrome neonatal
- respiratory distress syndrome of the newborn


 Assoziationen und Differentialdiagnosen zu acute respiratory distress syndrome (ARDS):
Assoziationen und Differentialdiagnosen zu acute respiratory distress syndrome (ARDS):