gastrointestinale Manifestationen Sklerodermie











Gastrointestinal manifestations of scleroderma can occur in up to 90% of patients with scleroderma with the most common site of gastrointestinal involvement being the esophagus. After skin changes and Raynaud phenomenon, gastrointestinal changes are the third most common manifestation of scleroderma.
As the clinical presentation, radiographic appearances and differential diagnosis vary with the location of involvement these are discussed sequentially by region.
For a general discussion of scleroderma, please refer to the parent article: scleroderma.
Pathology
Smooth muscle atrophy and fibrosis are thought to be the chief underlying mechanism which leads to luminal dilatation, reduced motility and reduced sphincter tone.
Esophagus
The esophagus is affected in 80% of scleroderma cases. Symptoms include heartburn and dysphagia.
Radiographic features
- dilatation of distal two-thirds of the esophagus
- deficient esophageal emptying in a recumbent position
- apparent shortening of length due to fibrosis
- dysmotility of the lower esophagus (normal peristalsis above aortic arch)
- gastro-esophageal reflux due to reduced sphincter tone
- air-fluid level in the esophagus when supine (CT)
Complications
- aspiration
- esophagitis
- mucosal erosion
- fusiform stricture ~4-5 cm above the gastro-esophageal junction
- progression to Barrett esophagus (~40%)
- higher risk of development of esophageal cancer (adenocarcinoma)
Differential diagnoses
The differential diagnosis includes other causes of a dilated esophagus (see achalasia pattern) and includes:
- achalasia: distal segment narrowing is less than 3.5 cm
- central and peripheral neuropathy
- esophageal malignancy
- esophageal stricture
Stomach
Gastric involvement is relatively uncommon but can result in delayed gastric emptying with or without gastric dilatation. Gastric vascular antral ectasia (dilated submucosal capillaries), often known as watermelon stomach, may also occur.
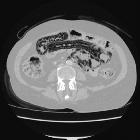
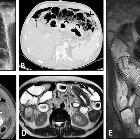
Small bowel
The small bowel is affected in more than 60% of scleroderma patients, the duodenum most frequently. Patients may be asymptomatic or may present with bloating or malabsorption due to bacterial overgrowth.
Radiographic features
- luminal dilatation (can be massive)
- reduced peristalsis / delayed contrast transit
- mucosal folds appear relatively normal despite dilatation
- hidebound bowel sign (crowding of valvulae conniventes): thought to be pathognomonic of scleroderma
- accordion sign: well seen evenly spaced mucosal folds in duodenum
- sacculation (often on the mesenteric border)
Differential diagnoses
- sprue: segmentation, flocculation, hypersecretion
- small bowel obstruction
Large bowel
The large bowel is affected in ~40% of patients and may cause constipation or diarrhea. Reduced anal sphincter tone can result in fecal incontinence.
Radiographic features
- pseudosacculation
- loss of haustration
- colonic dilatation
- reduced colonic transit time
Differential diagnosis
See also
- musculoskeletal manifestations of scleroderma
- pulmonary manifestations of scleroderma
- cardiac manifestations of scleroderma
- hepatobiliary manifestations of scleroderma
- renal manifestations of scleroderma
Siehe auch:
- Dünndarmileus
- Sklerodermie Ösophagus
- Achalasie
- Pseudoachalasie
- Systemische Sklerodermie
- Wandstarre unterer Ösophagus
- Ösophagusstrikur
- stack of coins
- Sprue
- Pneumatosis intestinalis bei Sklerodermie
- Morbus Hirschsprung beim Erwachsenen
- oesophageal cancer (adenocarcinoma)
- pseudo-obstruction
und weiter:


 Assoziationen und Differentialdiagnosen zu gastrointestinale Manifestationen Sklerodermie:
Assoziationen und Differentialdiagnosen zu gastrointestinale Manifestationen Sklerodermie: