hepatic cyst





Simple hepatic cysts are common benign liver lesions and have no malignant potential. They can be diagnosed with ultrasound, CT, or MRI.
Epidemiology
Simple hepatic cysts are one of the commonest liver lesions, occurring in ~2-7% of the population . There may be a slight female predilection.
Clinical presentation
Hepatic cysts are typically discovered incidentally and are almost always asymptomatic.
Pathology
Simple hepatic cysts may be isolated or multiple and may vary from a few millimeters to several centimeters in diameter. Simple hepatic cysts are benign developmental lesions that do not communicate with the biliary tree . The current theory regarding the origin of true hepatic cysts is that they originate from hamartomatous tissue. On histopathological analysis, true hepatic cysts contain serous fluid and are lined by a nearly imperceptible wall consisting of cuboidal epithelium, identical to that of bile ducts, and a thin underlying rim of fibrous stroma .
Location
While they can occur anywhere in the liver, there may be a greater predilection towards the right lobe of the liver .
Associations
Certain diseases are associated with multiple hepatic cysts and include
- polycystic liver disease
- autosomal dominant polycystic kidney disease (ADPKD): hepatic cysts may be seen in ~40% of those with ADPKD .
- von Hippel Lindau disease
Radiographic features
They are typically round or ovoid in shape and have well-defined margins. The cyst wall is very thin or even imperceptible .
Ultrasound
- round or ovoid anechoic lesion (may be lobulated)
- well-marginated with a thin or imperceptible wall and a clearly defined back wall
- may show posterior acoustic enhancement, if large enough
- a few septa may be possible, but no wall thickening
- a small amount of layering debris is possible
- no internal vascularity on color Doppler
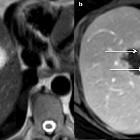
CT
On CT, a hepatic cyst demonstrates homogeneous hypoattenuation (water attenuation) around 0-10 HU. The wall is usually imperceptible, and the cyst does not enhance after intravenous administration of contrast material.
MRI
On MR imaging a hepatic cyst follows the signal intensity of water on all sequences:
- T1: homogeneous very low signal intensity
- T2: increased signal intensity, greater than other T2 hyperintense liver lesions (e.g. hemangioma)
- T1 C+: hepatic cysts do not enhance after administration of any type of contrast
In instances of intracystic hemorrhage, which is a rare complication in simple hepatic cysts, the signal intensity is high and heterogeneous, with a fluid-fluid level on both T1- and T2-weighted images when mixed-blood products are present . Also, elevated T1 signal can be seen in proteinaceous content. For both these circumstances, using imaging subtraction can be essential when assessing for the presence of enhancement.
Differential diagnosis
General imaging differential considerations include other cystic liver lesions, including:
- hepatic hydatid cyst(s)
- hepatic abscess(es)
- hepatic biloma
- biliary cystadenoma(s)
- choledochal cyst: communicates with the biliary tree
- necrotic hepatic metastasis (would probably have lower T2 than a cyst, higher CT attenuation, and enhancement of a thickened wall)
On CT and T2 MRI images also consider:
On the LI-RADS classification system, a simple cyst is given a designation of LR1 or LR2.
Siehe auch:
- Leberabszess
- Echinococcus Leber
- Choledochuszyste
- Von-Meyenburg-Komplex
- Lebermetastasen
- Differenzialdiagnosen zystischer Leberläsionen
- eingeblutete Leberzyste
- zystische Lebermetastasen
- biliäres Zystadenom
- Zystenleber
und weiter:


 Assoziationen und Differentialdiagnosen zu simple Leberzyste:
Assoziationen und Differentialdiagnosen zu simple Leberzyste: