thoracic empyema





























Pleural-thoracic empyema (commonly referred simply as an empyema) or pyothorax refers to an infected purulent and often loculated pleural effusion, and is a cause of a large unilateral pleural collection. It is a potentially life-threatening condition requiring prompt diagnosis and treatment.
Epidemiology
Empyemas are usually the complication of another underlying abnormality, and thus demographics will follow those of the primary cause, e.g. pneumonia, sub-diaphragmatic abscess, esophageal perforation etc...
Patients with HIV/AIDS are more likely to have pneumonia, and in turn are more likely to develop an empyema, which may occur in >5% of cases of pneumonia .
Clinical presentation
Clinical signs and symptoms in isolation are non-specific, and mimic pulmonary infection of any compartment, with fever and increased white cell count being common.
In the setting of a pleural collection, consolidation and infective symptoms, imaging alone is unable to exclude infection, and thoracocentesis with microbiological assessment is required. Presence of gas locules within the collection or thickened enhancing pleural margins are strongly indicative of infection (see below).
Additionally, the presumptive diagnosis can be made if the fluid pH is <7.0 or the fluid has a glucose level <40mg/dL .
Pathology
Microbiology
Offending organisms vary somewhat according to the age at which the empyema develops and the underlying abnormality / primary site of infection. For parapneumonic empyemas most frequent organisms are :
- childhood
- Pneumococcus
- adults
- penicillin-resistant Staphylococcus aureus
- gram-negative bacteria
- anaerobic bacteria: usually polymicrobial
In the setting of trauma or thoracic surgery, Staphylococcus aureus is usually involved .
Other uncommon causes include
mycobacterial infection
Specific subtypes
Radiographic features
Plain radiograph
Can resemble a pleural effusion and can mimic a peripheral pulmonary abscess, although a number of features usually enable distinction between the two (see empyema vs lung abscess) . Pleural fluid is typically unilateral or markedly asymmetric . Generally, empyemas form an obtuse angle with the chest wall, and due to their lenticular shape are much larger in one projection (e.g. frontal) compared to the orthogonal projection (e.g. lateral) . The lenticular shape (biconvex) is also suggestive of the diagnosis, as transudative/sterile pleural effusions tend to be crescentic in shape (i.e. concave towards the lung, see empyema vs pleural effusion).
Ultrasound
The appearances of an empyema depend on the composition of the collection. Typically they are not uniformly anechoic and are often septated.
Ultrasound has a major role in enabling targeted thoracocentesis.
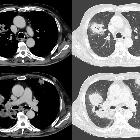
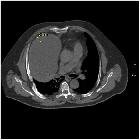
CT
Typically appears as a fluid density collection in the pleural space, sometimes with locules of gas. They form obtuse angles with the adjacent lung, which is displaced and compressed. The pleura is thickened due to fibrin deposition and in-growth of vessels with enhancement. At the margins of the empyema, the pleura can be seen dividing into parietal and visceral layers, the so-called split pleura sign, which is the most sensitive and specific sign on CT, and is helpful in distinguishing an empyema from a peripheral lung abscess (see: empyema vs lung abscess) . The inner walls of the empyema are smooth.
Treatment and prognosis
Prompt evacuation of the infected fluid along with appropriate antibiotics is the mainstay of treatment and will not only improve survival but also hopefully prevent the formation of a fibrothorax.
Evacuation may be performed with percutaneous chest tube placement often with an administration of a fibrinolytic agent (e.g. streptokinase or urokinase ) into the pleural space to break down septations. Alternatively, video-assisted thoracic surgery (VATS), open decortication, or even Clagett thoracotomy may be performed. VATS is increasingly thought to lead to faster resolution with lower morbidity and reduced cost .
Prognosis is not surprisingly worse in HIV/AIDS patients with reduced CD4 counts .
History and etymology
Baron Guillaume Dupuytren (of Dupuytren contracture fame) Bonaparte died of empyema in 1835 .
Differential diagnosis
General imaging differential considerations include
- pleural effusion from other causes, especially in the setting of inflammatory conditions
- systemic lupus erythematosus (SLE)
- rheumatoid arthritis
- Dressler syndrome (post-myocardial infarction)
- hiatus hernia (AP film)
- lung abscess: see empyema vs lung abscess
- cavitating lung lesion
See also
- pyopneumothorax: can be thought of a subtype of an empyema
Siehe auch:
- Pleuraerguss
- Hiatushernie
- Kavernöse Lungenläsionen
- Lungenabszess
- Pleurakarzinose
- systemischer Lupus Erythematodes
- Pleuramesotheliom
- Clagett thoracotomy
- Empyema necessitans
- eitrige Perikarditis
- thorakale Aktinomykose
- extrapleurales Hämatom
- gekammerter Pleuraerguss
- Eloesser flap
- Pleuraempyem vs. Lungenabszess
- Pleuraempyem Kontrastmittelaufnahme
- tuberkulöses Pleuraempyem
- Unterscheidung Pleuraerguss - Pleuraempyem
und weiter:


 Assoziationen und Differentialdiagnosen zu Pleuraempyem:
Assoziationen und Differentialdiagnosen zu Pleuraempyem: