Joubert-Syndrom

























Joubert anomaly, also known as vermian aplasia or molar tooth midbrain-hindbrain malformation, is an autosomal recessive disorder where there is a variable degree of cerebellar vermal agenesis.
Terminology
When associated with anomalies of the kidneys, liver and/or eyes then the term Joubert syndrome and related disorders (JSRD) is used.
Epidemiology
The prevalence of Joubert syndrome is approximately 1 in 100,000. There are numerous associations which are variably present :
- ocular abnormalities
- coloboma
- retinal dysplasia: 50%-some authors advocate dividing Joubert syndrome patients into two groups according to the presence or absence of retinal dysplasia
- nephronophthisis
- multicystic dysplastic kidneys (MCDK): 30%
- hepatic fibrosis - usually as part of COACH syndrome
- polydactyly: 15%
- Occipital (meningo) encephalocele
Clinical presentation
Affected individuals usually present with ataxia and have dysmorphic facies, global developmental delay, hypotonia, rapid breathing and oculomotor apraxia. There is significant range in the degree of cognitive impairment with IQ ranging from 30 to 80, although presence of speech and motor deficits makes assessment difficult .
Typically, patients have nystagmus and inability of smooth pursuit of a moving object .
Pathology
Joubert syndrome patients are a heterogeneous population in terms of genetics with some having a mutation of chromosome 9q34.3; many do not . At least 10 genes have been implicated, relating to subcellular organelle the primary cilium and basal body; as such JS is one of a number of related disorders known as ciliopathies .
Radiographic features
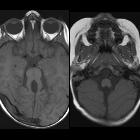
Cross-sectional axial imaging demonstrates isolated abnormality of the cerebellum, consisting of:
- small dysplastic or aplastic cerebellar vermis
- absence of fiber decussation in the superior cerebellar peduncles and pyramidal tracts , which can be assessed by diffusion tensor imaging
- abnormal inferior olivary nucleus
- dysplasia and heterotopia of cerebellar nuclei
The posterior fossa typically shows a bat wing 4 ventricle and prominent thickened elongated superior cerebellar peduncles giving characteristic molar tooth like appearance.
In a minority of cases minor lateral ventriculomegaly (6 - 20% of cases), and corpus callosal dysgenesis (6-10% of cases) is also present .
Treatment and prognosis
Not an overwhelming amount of data is available on the long term outcome of children with Joubert syndrome. Persistent neuromotor developmental retardation is a feature of surviving individuals. Patients with associated retinal dysplasia appear to have a poorer prognosis .
Extreme care needs to be taken when administering any agent that causes respiratory depression, as individuals with Joubert syndrome are exquisitely sensitive to these effects .
Genetic counseling is required as the condition is autosomal recessive.
History and etymology
It is named after the French neurologist: Marie Joubert who first described the condition in 1969.
Differential diagnosis
The differential for Joubert syndrome include:
- Dandy-Walker malformation: the Dandy-Walker continuum may also occur simultaneously with the Joubert anomaly in some cases
- rhombencephalosynapsis
- mega cisterna magna: no structural abnormality
Siehe auch:
- Mega Cisterna magna
- Mesencephalon
- Dandy-Walker-Syndrom
- Rhombencephalosynapsis
- Backenzahn-Zeichen (ZNS)
- Cogan-Syndrom
- Dysgenesie des Vermis
- molar tooth sign - abdominal
und weiter:
- Polydaktylie
- Dandy-Walker continuum
- animal and animal produce inspired signs
- neuroradiologisches Curriculum
- COACH syndrome
- classification system for midline abnormalities of the brain and skull
- classification system for malformations of the cerebellum
- zerebelläre Anomalien
- Varadi-Papp-Syndrom
- Renales-Kolobom-Syndrom
- bat wing 4th ventricle
- zystische Malformationen der hinteren Schädelgrube
- Nathalie-Syndrom
- batwing fourth ventricle


 Assoziationen und Differentialdiagnosen zu Joubert-Syndrom:
Assoziationen und Differentialdiagnosen zu Joubert-Syndrom:



