mediastinal lymphoma
Mediastinal lymphoma is common, either as part of disseminated disease or less commonly as the site of primary involvement.
Epidemiology
Lymphomas are responsible for approximately 15% of all primary mediastinal masses, and 45% of anterior mediastinal masses in children . Only 10% of lymphomas which involve the mediastinum are primary (i.e. mediastinal involvement not part of systemic disease) and the majority are Hodgkin lymphomas (~ 60%) .
Clinical presentation
The mediastinum is commonly involved in systemic lymphomas. Approximately 60% of all Hodgkin lymphoma and 20% of non-Hodgkin lymphoma involves the mediastinum at presentation. Less frequently, the disease is isolated to the mediastinum (3% Hodgkin lymphoma, <10% non-Hodgkin lymphoma) . As such, patients are often asymptomatic from the mediastinal component but present with systemic manifestations of lymphoma, most commonly constitutional symptoms .
Symptoms directly attributable to the mediastinal component include :
- retrosternal chest pain
- SVC compression with SVC syndrome
- dyspnea
- cough
Pathology
Mediastinal lymphomas usually arise from either the thymus or lymph nodes, thus accounting for their predilection for the anterior and middle mediastinum . The anterior mediastinal and para-tracheal nodes are the most frequently involved regions while isolated hilar node enlargement is uncommon without accompanying mediastinal node enlargement. Posterior mediastinal involvement is also infrequent.
Current World Health Organization classification of neoplastic diseases of the lymphoid tissues includes lymphomas and leukaemias, and is according to the cell of origin, with the main division being:
- B-cell neoplasms
- T-cell and natural killer cell neoplasms
- Hodgkin lymphoma
Primary mediastinal lymphomas are most frequently of three histologic varieties :
Radiographic features
The majority of patients have anterior mediastinal and paratracheal involvement. Isolated hilar nodal involvement is uncommon .
Plain radiograph
A soft tissue mass may be clearly visible, or more frequently the mediastinum is widened, and the retrosternal airspace is obscured.
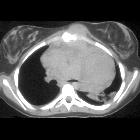
CT
CT demonstrates a soft tissue attenuating mass, with smooth or lobulated margins which conform to surrounding structures. Cystic/ low-density areas are common. Other features include :
- parenchymal invasion: uncommon
- pleural effusion(s)
- seen in 50% of cases
- usually unilateral
- usually exudates
- pleural deposits may be present
- pericardial effusion
- chest wall invasion
Calcification is usually seen following therapy and can have varying morphology, including irregular, diffuse or even egg-shell .
Following treatment nodal masses usually reduce in size, however in some instances the size of the mass remains the same or even increases (in cases of thymic hyperplasia) . As such CT is not ideal for assessing for treatment response when a decrease in size is not present.
MRI
Appearance of lymphomas on MRI varies with treatment and type of lymphoma .
- T1: replace
- T2
- at diagnosis: variable but present
- following treatment: decreases
- T1 C+ (Gd)
- at diagnosis: variable but present
- following treatment: decreases and becomes more heterogeneous due to necrosis and fibrosis
- absence of decrease following treatment suggests the continued presence of viable neoplastic tissue
Gallium and FDG-PET
Both gallium-67 scintigraphy and FDG-PET are better able to assess for tumor viability following treatment than CT, as residual mass does not necessarily represent residual viable neoplastic tissue .
Unfortunately, up to 20% of cases are gallium negative at diagnosis .
Treatment and prognosis
Specific treatment depends on the type of lymphoma and the stage, but broadly requires chemotherapy and or radiotherapy .
Similarly, the prognosis is very variable. Stage I and II Hodgkin lymphoma have the best prognosis with a greater than 90% cure rate .
Complications
Complications include:
- vascular compression
- SVC syndrome
- compression of the aorta
- compression of the pulmonary arteries
Differential diagnosis
On chest radiography, the differential is that of mediastinal lymph node enlargement and of an anterior mediastinal mass.
On CT the differential includes:
- thymic tumors
- mediastinal germ cell tumors
- sarcoidosis
- infection: especially tuberculosis
Siehe auch:
- Tuberkulose
- Perikarderguss
- Pleuraerguss
- Sarkoidose
- Thymus
- Tumoren des vorderen oberen Mediastinums
- vordere Schulterluxation
- Thymushyperplasie
- Morbus Hodgkin
- primary mediastinal large B-cell lymphoma
- mediastinale Keimzelltumoren
- Obere Einflussstauung
- Tumoren des Thymus
- retrosternal airspace is obscured
- egg-shell
- World Health Organisation classification of neoplastic diseases of the lymphoid tissues
- Stage I and II Hodgkin lymphoma
und weiter:


 Assoziationen und Differentialdiagnosen zu mediastinal lymphoma:
Assoziationen und Differentialdiagnosen zu mediastinal lymphoma: