pineocytoma








Pineocytomas are a relatively benign pineal parenchymal tumor that have a relatively good prognosis.
On imaging, they generally appear as a well-demarcated tumor with less than 3 cm, iso to hyperattenuating on CT, hypo to isointense on T1, and hyperintense on T2. An avid and homogeneous enhancement is characteristic. Cystic changes may be present, which in some cases, can make difficult the differentiation from a pineal cyst.
Epidemiology
Pineocytomas can be encountered at any age but mostly occur in adults (20-60 years of age) . Unlike pineal germinomas, which have a strong predilection for males, pineocytomas are somewhat more frequently encountered in females (M:F 0.6:1).
Clinical presentation
As with all other pineal region masses, clinical presentation is mainly from obstructive hydrocephalus secondary to compression of the tectum of the midbrain and obstruction of the aqueduct. Compression of the superior colliculi can also lead to a characteristic gaze palsy, known as Parinaud syndrome.
Pathology
Pineocytomas are well-differentiated tumors and considered a WHO grade I tumors in the current WHO classification of CNS tumors, believed to arise from pinealocyte .
Macroscopic appearance
These tumors are well circumscribed, with cystic or hemorrhagic change sometimes evident . They have a grey or tan cut surface.
Microscopic appearance
Under light microscopy, pineocytomas are composed of small cells similar in appearance to normal pinealocytes, arranged in sheets; pineocytomatous pseudorosettes are characteristic and not seen in normal pineal gland tissue .
As is the case with the rest of the pineal gland, pineocytomas do not have a well-formed blood brain barrier and as such enhance vividly with contrast .
Immunophenotype
- synaptophysin: positive
- neurofilament: positive
- neuron-specific enolase: positive
- other neuronal markers (e.g. MAPT, chromogranin-A, 5-HT etc..): variable
- NeuN: negative
Radiographic features
Typically pineocytomas are slow growing and well-circumscribed tumors (compared to pineoblastomas that tend to be larger, and less well-circumscribed). They tend to be solid, although focal areas of cystic change, or hemorrhage do occur. When the cystic component is large, distinguishing them from pineal cysts can be difficult, although it has been postulated that this is not so much the case if complete and accurate imaging is obtained (i.e. good quality thin section MRI with contrast) .
CT
CT demonstrates the mass to be of intermediate density, similar to the adjacent brain. Pineal calcifications tend to be dispersed peripherally. This is the same pattern seen in other pineal parenchymal tumors, which is helpful in distinguishing these tumors from pineal germinomas that tend to 'engulf' pineal calcification.
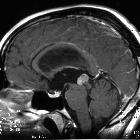
MRI
MRI is the modality of choice for examining tumors of the pineal region.
- T1: hypo to isointense to brain parenchyma
- T2
- solid components are isointense to brain parenchyma
- areas of cystic change are common
- sometimes the majority of the tumor is cystic
- T1 C+ (Gd): solid components vividly enhance
Treatment and prognosis
Pineocytomas are treated surgically and have an excellent prognosis when a complete resection is achieved (which is most of the time as they are well-circumscribed lesions). A 5-year survival of 86% has been reported .
Local recurrent and even CSF metastases are reported, but rare .
Differential diagnosis
On CT or MRI consider:
- pineal cyst
- at most thin smooth (<2 mm) peripheral enhancement
- other pineal parenchymal tumors
- germ cell tumors
- germinoma
- marked male predominance
- engulfed calcification
- embryonal carcinoma
- choriocarcinoma
- teratoma: may contain fat
- germinoma
- astrocytoma of the pineal gland
- metastasis
Siehe auch:
- Teratom
- Pinealiszyste
- WHO-Klassifikation der Tumoren des zentralen Nervensystems
- Astrozytom
- Tumoren der Pinealisregion
- Germinom
- Pineoblastom
- Keimzelltumor
- Verschlusshydrocephalus
- Parenchymtumor der Glandula pinealis mit intermediärer Differenzierung
- Papillärer Tumor der Pinealisregion
- Aquäduktsyndrom
- Parenchymtumoren der Glandula pinealis
und weiter:


 Assoziationen und Differentialdiagnosen zu Pineozytom:
Assoziationen und Differentialdiagnosen zu Pineozytom: