pineal cyst






















Pineal cysts are common, usually asymptomatic, and typically found incidentally. Their importance is mainly in the fact that they cannot be distinguished from cystic tumors, especially when large or when atypical features are present. As such, many patients undergo prolonged follow-up for these lesions, presumably with associated anxiety.
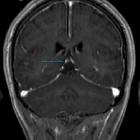
They generally present as a unilocular cyst within the pineal gland, where attenuation or fluid signal may vary from similar to CSF to around 60% being slightly hyperintense to CSF on T1 weighted images. A thin, smooth rim of contrast enhancement is seen in most cases and calcifications are present in 25% of instances.
Epidemiology
Pineal cysts are typically found in young aged adults (20-30 years of age) with a predilection for women (3:1 female to male ratio). They are seen in ~5% of brain MRIs and 20-40% of autopsy series. In high-resolution MRIs, a study found a high prevalence of asymptomatic cysts in 23% of healthy subjects .
Clinical presentation
The vast majority of pineal cysts are small (<1 cm) and asymptomatic. When larger they can present with mass effect on the tectal plate leading to compression of the superior colliculi and Parinaud syndrome. If the cerebral aqueduct is compressed, they may also result in obstructive hydrocephalus. Rarely, hemorrhage into a pineal cyst can cause rapid expansion and so-called pineal apoplexy.
Pathology
Pineal cysts are composed of three concentric layers:
- inner layer: finely fibrillary glial tissue often containing hemosiderin
- middle layer: pineal parenchyma with or without calcification
- outer layer: thin fibrous connective tissue
As they are most frequently seen in young women, it has been suggested that hormonal changes play a part in their formation. As these women get older the cyst initially enlarges and then shrinks. In males, they tend to remain stable over time.
The cyst typically contains proteinaceous fluid that, as a result, does not follow CSF on imaging. Internal hemorrhage may also be present.
As is the case with the rest of the pineal gland, the walls of pineal cysts do not have a well-formed blood brain barrier, and as such, can enhance vividly with contrast .
Radiographic features
CT
Well circumscribed fluid density lesions with thin rim calcification seen in ~25% . Thin, smooth peripheral enhancement is also often seen. The internal cerebral veins are elevated and splayed by the cyst.
MRI
- T1
- typically iso to hypointense compared to brain parenchyma
- 55-60% are somewhat hyperintense when compared to CSF
- usually homogeneous in signal
- T2
- high signal
- usually slightly hypointense to CSF
- FLAIR: high signal does not often suppress fully
- DWI/ADC: they demonstrate no restricted diffusion
- T1 C+ (Gd)
- ~ 60% of lesions enhance
- enhancement is usually thin (<2 mm), smooth and confined to the rim (either complete or incomplete)
- it is important to note that if postcontrast imaging is delayed (60-90 min), gadolinium may diffuse into the cyst fluid and may lead to the mass appearing solid
- in atypical cases enhancement may be nodular, or there may be evidence of previous hemorrhage into the cysts
Treatment and prognosis
In almost all cases no treatment is necessary, and in most cases, provided that the cyst is small, no imaging follow-up is required.
In a study of 32 patients with pineal cyst, followed up from 6 months to 9 years, cyst enlargement was found in only 3 patients, with 75% remaining the same and the rest shrinking. The authors concluded that cysts with typical features may be followed up clinically, rather than with imaging .
When cysts are above 10-12 mm in diameter, follow-up imaging may be necessary, as a cystic pineocytoma may appear similar.
Differential diagnosis
Unfortunately, especially in the setting of nodular enhancement or incomplete imaging, it is not possible to distinguish a cystic pineocytoma from a pineal cyst on imaging alone, although if thorough imaging is carried out, most cases can be sorted out . If a cyst is larger than 10-12 mm many would advocate follow-up to ensure stability over time, although this is contentious.
Additionally, there are several other neoplasms that may arise in the pineal region, such as germ cell tumors (germinoma, embryonal carcinoma, choriocarcinoma, teratoma), pineocytoma, and metastases. These tumors may contain cystic elements and several are highly malignant, making the follow-up of a large or atypical cyst necessary.
The differential therefore includes:
- pineal parenchymal tumors:
- epidermoid cyst
- arachnoid cyst: these are usually posterior to the pineal gland
- germ cell tumors:
- cerebral metastasis
- vein of Galen aneurysm
For a complete list, see pineal mass article.
Siehe auch:
- Arachnoidalzyste
- verkalktes Corpus pineale
- Hirnmetastase
- Teratom
- intrakranielle Epidermoidzyste
- Tumoren der Pinealisregion
- epidermale Inklusionszyste
- Germinom
- Pineozytom
- Chorionkarzinom
- Keimzelltumor
- Parenchymtumoren der Glandula pinealis
- Embryonales Karzinom
und weiter:
- Glandula pinealis
- Pineoblastom
- cavum vergae cyst
- intraventricular epidermoid
- Apoplex der Glandula pinealis
- Cavum veli interpositi Zyste
- Pinealisinfarkt
- Epidermoidzyste der Glandula pinealis
- Pinealiszyste eingeblutet
- Pinealiszyste Differentialdiagnose
- pineal cyst complicated by haemorrhage
- multiloculated pineal cyst


 Assoziationen und Differentialdiagnosen zu Pinealiszyste:
Assoziationen und Differentialdiagnosen zu Pinealiszyste:









